Angina Pectoris Despite Normal Coronary Angiography: Need for Specialist Care
A 32-year-old female patient is experiencing frequent episodes of exertional and rest chest pain. The relationship between chest pain and effort is inconsistent, with some episodes occurring with minor exertion and others during strenuous exercise only. The episodes are typical in character and radiation but generally prolonged in duration and not necessarily associated with ECG changes. She also reports nocturnal episodes of chest pain which are relieved by sublingual nitrate administration. She denies symptoms of orthopnea, paroxysmal nocturnal dyspnea, pedal edema, pre-syncope, syncope, or palpitations. The patient has a history of transient visual loss and headaches. She does not have classical atherosclerotic risk factors.
|
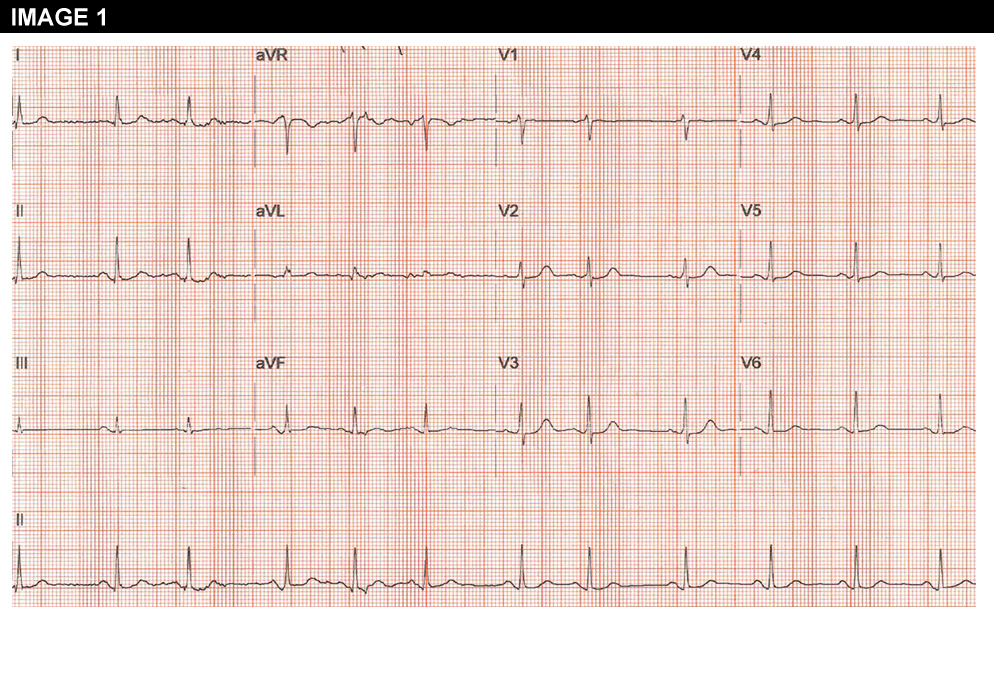
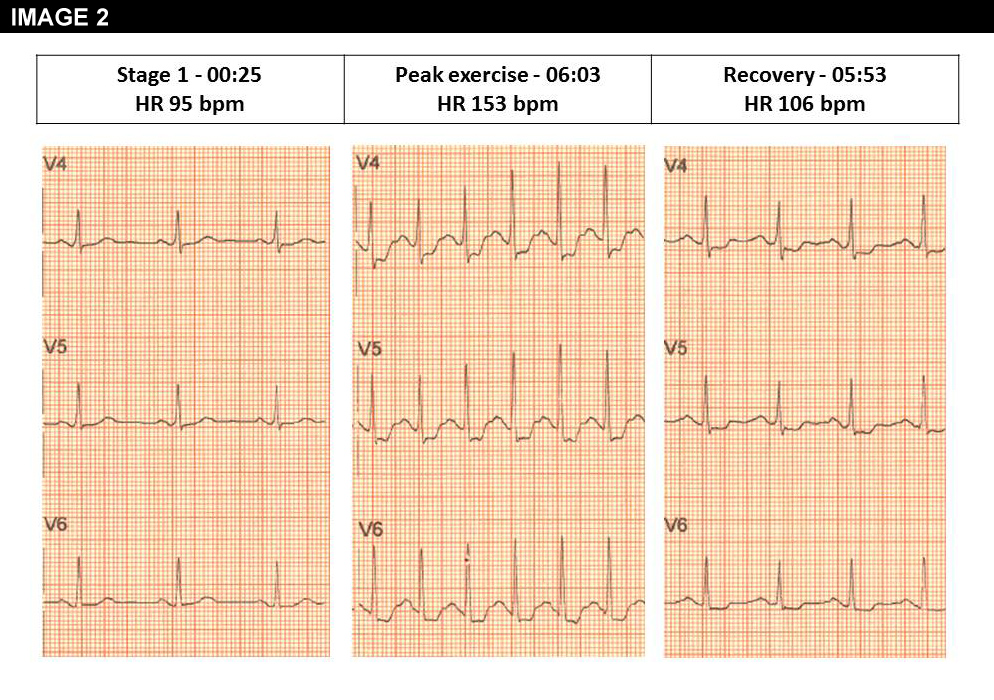

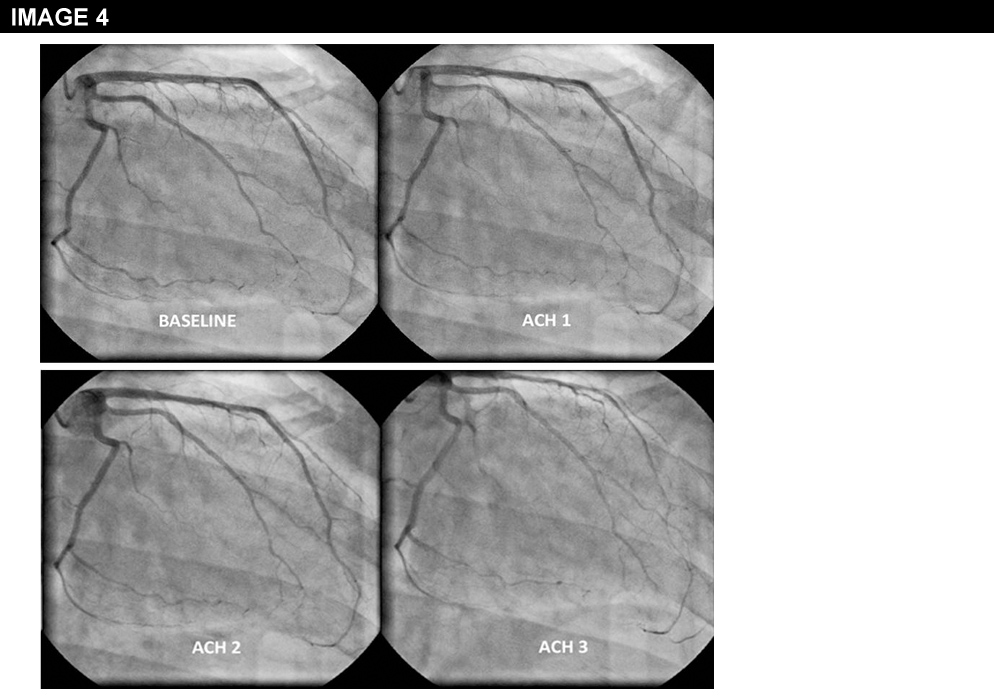


Physical examination is unremarkable. The resting ECG is normal with no ischaemic features (Image 1). She was referred for an ECG exercise stress test. She exercised for 6 min 35 seconds (Bruce protocol), achieved 131% of her heart rate and developed chest pain and breathlessness at peak exercise. Ischemic ST changes were noted which resolved slowly during recovery (Image 2). The patient was referred for cardiac catheterization which showed smooth unobstructed coronary arteries (Image 3). Provocation testing with acetylcholine was performed during angiography when incremental doses of acetylcholine 2mcg, 40mcg, 100mcg were injected in the left coronary system. This resulted in the reproduction of her symptoms, ST depression on the ECG and >75% diffuse epicardial coronary artery spasm of the left coronary artery (Image 4). The diameter of the coronary arteries returned to baseline after intracoronary nitrate administration and both the chest pain and the ECG changes subsided rapidly. Given the diffuse involvement of the distal segments of the coronary artery during the acetylcholine infusion, suggesting the presence of microvascular dysfunction, the patient underwent cardiac magnetic resonance perfusion scanning. Following adenosine stress, which reproduced her usual symptoms, the patient developed subendocardial hypoperfusion of the basal-mid inferior wall & adjacent septum & lateral wall with a circumferential pattern suggestive of microvascular angina (Image 5). On late gadolinium enhancement imaging there was no fibrosis or infarct (Image 6).
A diagnosis of coronary artery spasm and microvascular dysfunction was made and the patient was started on a calcium channel blocker. Both the intensity and frequency of her symptoms improved and the patient returned to her normal every-day activities. While on medical treatment, the patient underwent repeat stress perfusion cardiac magnetic resonance testing. The infusion of adenosine triggered some chest discomfort but no typical chest pain or perfusion defects occurred during the perfusion scan.
Please indicate–for this particular patient with chest pain and normal coronary arteries– which of the following statements is correct:
Show Answer