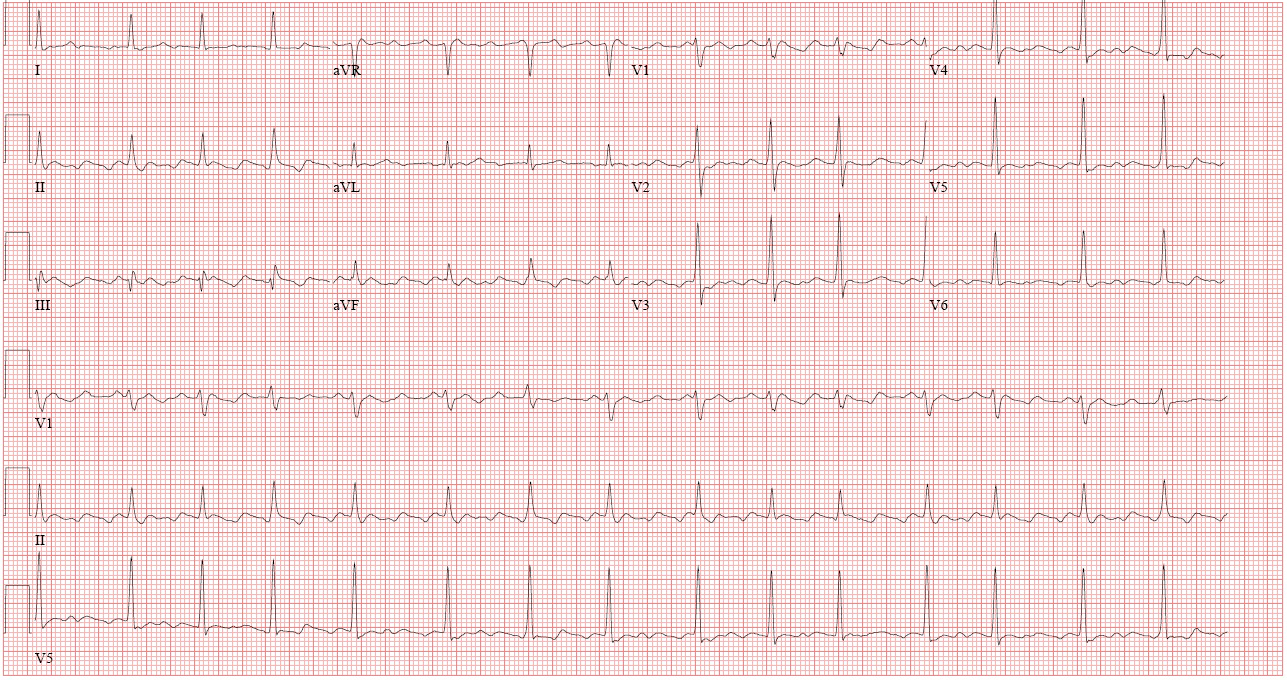
A 46-year-old male with a history of hypertension and hyperlipidemia presented to the emergency department with "stabbing chest pain." He was found to be in atrial fibrillation with rapid ventricular response. No imaging was performed, but he was started on sotalol and rivaroxaban. He was discharged but presented again three days later with fatigue and continued chest pain. He was found to be significantly bradycardic; thus, sotalol was discontinued, and a combination of flecainide and diltiazem were started. Two weeks after this, he again presented with continued, worsening chest pain. Coronary angiography was reportedly normal. Computed tomography of the chest, abdomen, and pelvis was performed after this, which showed a pericardial effusion; inflammatory markers were checked and were found to be significantly elevated. A diagnosis of pericarditis was made. He was transferred to our center for evaluation of the same. On arrival, he was tachycardic, with a heart rate of 114, with jugular venous distension to the angle of the mandible, trace peripheral edema, and an audible pericardial "knock." Renal function was normal, hemoglobin was normal, c-reactive protein was elevated at 79mg/L, erythrocyte sedimentation rate was elevated at 42mm/hr, brain natriuretic peptide was 435pg/mL, and troponins were negative. Rheumatologic evaluation was unrevealing. His presenting electrocardiogram showed atrial flutter (Figure 1). Magnetic resonance imaging (Figures 2 and 3) showed a moderate, circumferential pericardial effusion, thickening of the visceral and parietal pericardial layers, and circumferential increased pericardial signal intensity.
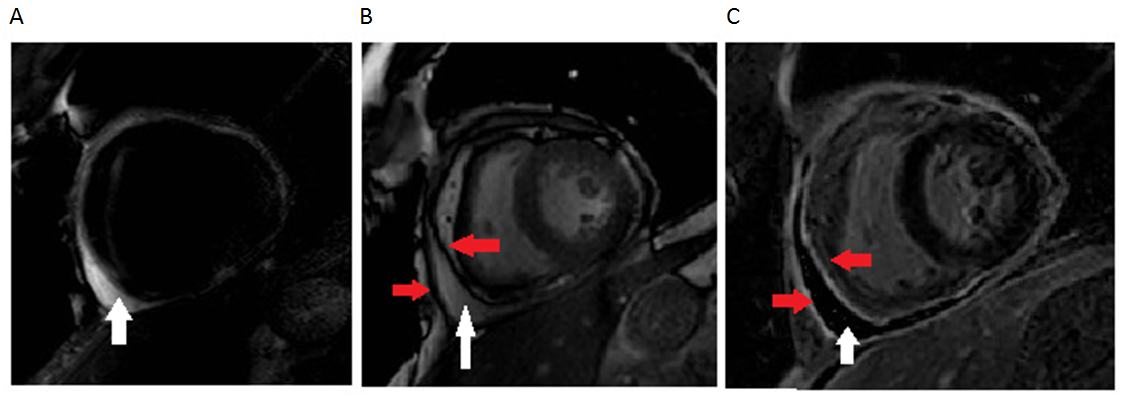
Figure 2A-C: Cardiac magnetic resonance imaging of the heart in a basal short axis slice using an A) T2 Short Tau Inversion Recovery [STIR] edema weighted sequence, B) steady-state free procession [SSFP] cine sequence and C) fat suppressed delayed enhancement imaging. A pericardial effusion is noted (white arrow), which limits the ability to differentiate concurrent pericardial edema using STIR imaging. The visceral and parietal pericardia are noted on cine imaging and moderately enhance on delayed enhancement imaging (red arrows).
Figure 3
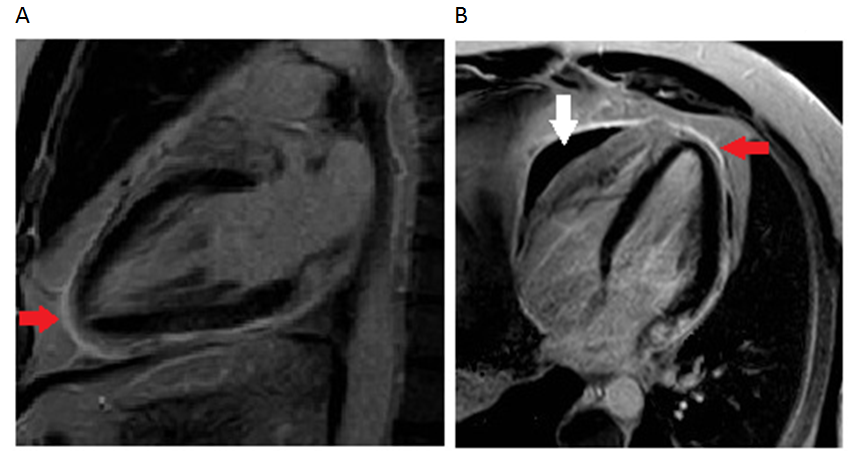
Figure 3: Phase-Sensitive Inversion Recovery [PSIR] Delayed Enhancement imaging in A) Vertical Long Axis [VLA]) and B) Horizontal Long Axis [HLA]) views. Moderate pericardial delayed enhancement is noted (red arrow), with the pericardial effusion most prominent anteriorly (white arrow).
The patient was started on prednisone 60mg daily, ibuprofen 600mg thrice daily, and colchicine 0.6mg thrice daily with some relief of his pain; however, his atrial fibrillation persisted with rates maintained in the low 100s despite maximal doses of metoprolol. He had tolerated anticoagulation with intravenous heparin with no bleeding or change in hemoglobin.
How should his anticoagulation be managed at discharge?
Show Answer
The correct answer is: B. Aspirin alone
Early case series of patients with acute pericarditis showed that these patients sometimes developed atrial arrhythmias, including atrial fibrillation1,2, an observation supported by a more recent study3. In these, incidence ranged from 4-7 percent.
For those in whom atrial fibrillation does occur, the use of systemic anticoagulation is controversial. A common concern is the development of tamponade in patients who have acute pericarditis and are anticoagulated. One series tracked 274 patients with acute pericarditis to determine what factors predicted tamponade; the authors found that anticoagulation with "heparin or other anticoagulants" was not associated with an increased risk of tamponade.4 Another study, following 453 patients with acute pericarditis, indicated that patients with complications (including tamponade) were three times as likely to have been on oral anticoagulants as those who had no complications (14.7% versus 4.0%, P<0.001) . A third, more recent study following 822 patients with acute pericarditis showed no increased risk of tamponade with the use of heparin or other oral anticoagulants (95% confidence interval 0.3-3.5, P=0.918).5
Interestingly, no American guidelines address the question of anticoagulation in pericarditis-induced atrial fibrillation. Recently released European guidelines indicate that use of oral anticoagulants is a minor predictor of a poor prognosis. Their recommendations include avoiding anticoagulation in patients with uremic or iatrogenic pericarditis but indicate that anticoagulation may be considered in other patients with acute pericarditis and atrial fibrillation.6 Based upon the available data, we tend to treat these patients with either aspirin or warfarin (depending on the patient's CHA2DS2-VASc score). As such, we placed this particular patient on high dose aspirin, using it as both an anticoagulant and an anti-inflammatory. In the year that we have been following him since his initial presentation, he has tolerated this well, without bleeding, and his effusion has resolved.
In summary, atrial fibrillation is seen in approximately five percent of patients with acute pericarditis. Patients with acute pericarditis should be anticoagulated based upon their risk for stroke, using one of the commonly available clinical decision tools. We tend to not use the NOACs, given the lack of evidence in this particular patient population. Thus, either 325mg aspirin or warfarin titrated to an INR of 2-3 are our preferred anticoagulants for patients with atrial fibrillation and acute pericarditis.
References
Spodick, DH. "Arrhythmias During Acute Pericarditis: A prospective study of 100 consecutive cases." JAMA. 1976;235(1):39-41.
Spodick, DH. "Frequency of arrhythmias in acute pericarditis determined by holter monitoring." Am J Cardiol. 1984;53(6):842-845
Imazio M, Lazaros G, Picardi E, et al. "Incidence and prognostic significance of new onset atrial fibrillation/flutter in acute pericarditis." Heart. 2015;101(18):1463-1467.
Imazio M, Cecchi E, Demichelis B, et al. "Myopericarditis versus viral or idiopathic acute pericarditis." Heart. 2008;94(4):498–501
Imazio M, Cecchi E, Demichelis B, et al. "Indicators of poor prognosis of acute pericarditis." Circulation. 2007;115(21):2739–2744.
Adler Y, Charron P, Imazio M, et al. "2015 ESC Guidelines for the diagnosis and management of pericardial diseases." Eur Heart J. 2015;36(42):2921-2964