A 65-year-old male with no significant medical history complained of acute onset chest pain, right eye vision loss and lightheadedness. Shortly after, he collapsed and bystanders initiated cardiopulmonary resuscitation. Upon arrival, Emergency Medical Services (EMS) found the patient unresponsive with a systolic blood pressure in the 60's. He had palpable pulses, was in a normal sinus rhythm and EMS placed an emergent central venous line and intravenous saline was initiated in the field.
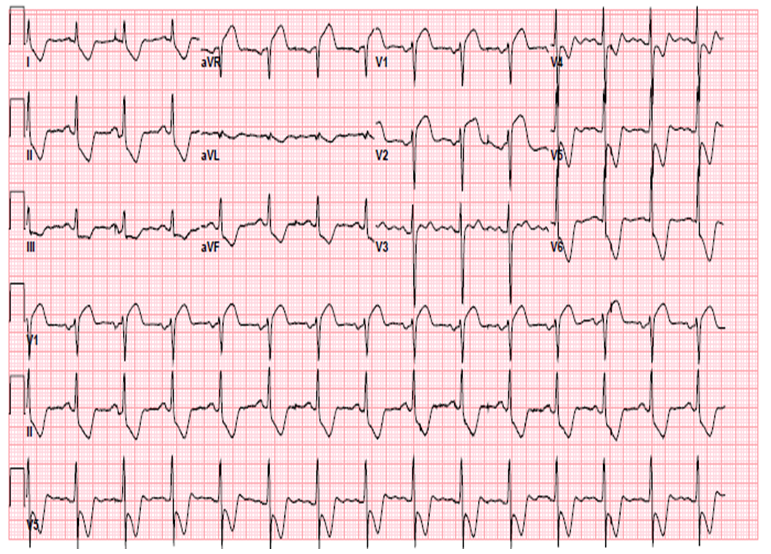
Upon arrival to the emergency department (ED), the patient was in respiratory distress, was intubated and placed on mechanical ventilation. Examination was notable for anisocoria with a dilated right pupil. Patient had a regular rate and rhythm with equal pulses and blood pressure readings bilaterally. Scattered crackles were noted on auscultation of the lungs bilaterally with no murmurs, extra heart sounds, jugular venous distention, or edema. Portable chest x-ray was without of evidence of mediastinal widening. Electrocardiogram demonstrated ST segment elevations anteriorly and in aVR with reciprocal depressions inferolaterally (Figure 1).
Figure 1
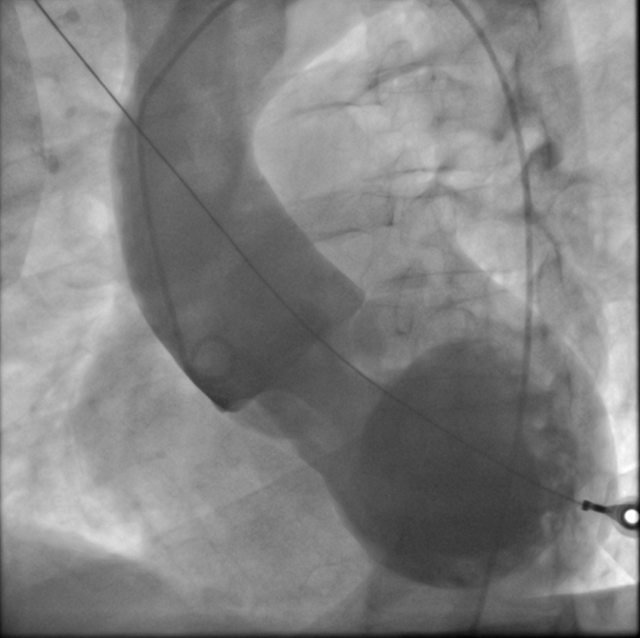
An ED bedside echocardiogram demonstrated a dilated aortic root with moderate aortic regurgitation without aortic intimal flap or regional wall motion abnormalities which were suggestive of acute aortic dissection (AAD). The patient was not hemodynamically stable enough to perform a computerized tomography scan (CT), so the decision was made to proceed directly with emergent aortography and potential angiography. An aortogram revealed a prolapsing proximal aortic dissection flap with aortic root dilatation and severe aortic regurgitation (Figure 2).
Figure 2
The patient was taken directly to the operating room, and underwent a successful type A aortic dissection repair with replacement of the ascending aorta and hemi-arch and re-suspension of the aortic valve. He was discharged to cardiac rehabilitation and had an uneventful post-operative course.
What percentage of patients with Type A acute aortic dissection present with ST segment elevation on their electrocardiogram (ECG)?
Show Answer
The correct answer is: B. 3-10%
Aortic dissection is a lethal disease for which an early and accurate diagnosis is critical1-6. A wide variety of clinical presentations often make aortic dissection difficult to diagnose, especially in the presence of electrocardiographic (ECG) changes that mimic acute coronary syndrome (ACS)1,2.
According to The International Registry of Acute Aortic Dissection (IRAD) study, ST segment elevation was found in 3.2% of aortic dissections and 4.7% of proximal dissections3. In a separate study, Hirata et al. focused on the presence of ECG changes in patients with type A acute aortic dissections, and found that 49.7% of patients who presented to the ED within 12 hours of symptom onset had some type of ECG abnormality4. The majority of acute ECG changes were nonspecific but 8.2% of patients presented with ST segment elevation4. In this study, the location of the ST elevation was found in the inferior leads (II, III, and aVF) in 7 patients, aVL and aVR in 2 patients, anterolateral leads (V1–V6, I aVL) in 2 patients and all the leads in 2 patients4.
Based on the current literature, the majority of ST segment elevation seen in AAD occurs in the inferior leads and often involves occlusion and malperfusion of the right coronary artery1,4. In our case, the patient presented with ST elevations anteriorly and in aVR. His ECG (Figure 1) is classic for anterior ST segment elevation MI (STEMI) with left main or proximal left anterior descending coronary artery involvement and aortic dissection may easily be missed.
Maintaining a clinical suspicion for aortic dissection is important for making an early accurate diagnosis and initiating emergency treatment1,5. Most importantly, it can prevent initiating ACS treatments including thrombolysis, anticoagulation, antiplatelet, or percutaneous catheter intervention, which may be potentially harmful in these patients5.
The initial imaging study used most frequently in acute aortic dissection is typically contrast-enhanced computed tomography, with magnetic resonance imaging and transesophageal echocardiography used in smaller numbers of patients1. While all of these modalities carry a similar high sensitivity and specificity, availability may be limited and could delay rapid diagnosis1,6. In hemodynamically unstable patients and in patients with ECG findings concerning for STEMI, aortography may be the most direct imaging modality to make a rapid and accurate diagnosis, without delaying treatment in the patient who instead has STEMI.
References
Braverman, A. Aortic Dissection: Prompt diagnosis and emergency treatment are critical. CCJM. 2011 Oct;78(10):685-696.
Cohen R, Mena D, Carbajal-Mendoza R, Arole O, Mejia JO. A case report on asymptomatic ascending aortic dissection. Int J Angiol. 2008 Autumn;17(3):155-161.
Hagan PG, Nienaber CA, Isselbacher EM et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000 Feb 16;283(7):897-903.
Hirata K, Wake M, Kyushima M et al. Electrocardiographic changes in patients with type A acute aortic dissection: Incidence, patterns and underlying mechanisms in 159 cases. Journal of Cardiology. 2010 Sep;56(2):147-153.
Hansen MS, Nogareda GJ, Hutchison SJ. Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. Am J Cardiol. 2007 Mar 15;99(6):852-6.
Rapezzi C, Longhi S, Graziosi M et al. Risk factors for diagnostic delay in acute aortic dissection. Am J Cardiol. 2008 Nov 15;102(10):1399-406.