A 62-year-old man with a history of highly symptomatic paroxysmal atrial fibrillation (AF) refractory to multiple antiarrhythmic drugs was referred for catheter ablation.
Pre-procedure imaging demonstrated normal LV function (LVEF 60%), a normal left atrial volume (32 mL/m2), and a standard pulmonary vein anatomy with 4 distinct pulmonary vein ostia.
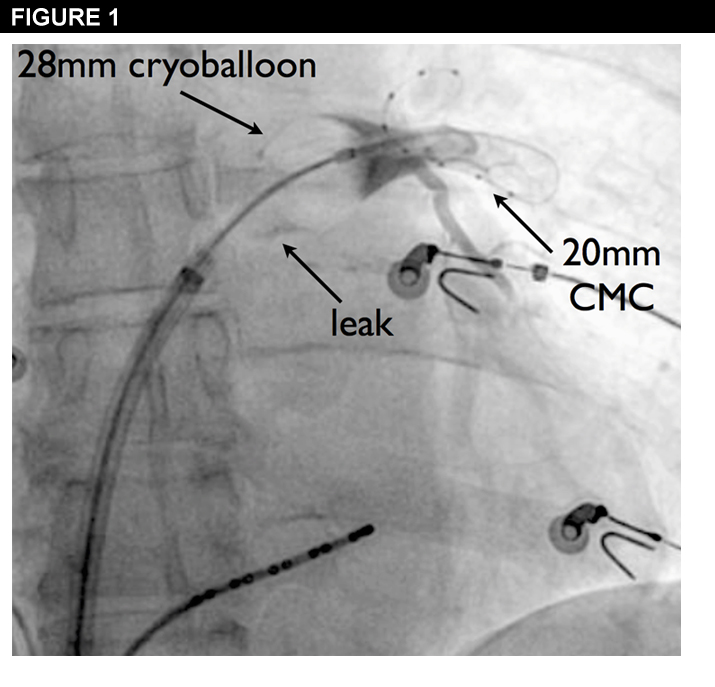
Shown in Figure 1 is the CB catheter, which is positioned at the ostium of the left superior pulmonary vein (LSPV). A 20 mm CMC is positioned inside the LSPV to ensure catheter stability and optimize PV ostium-cryoballoon contact. Despite the persistence of a small leak detected during pre-ablation contrast injection (Figure 1) cryoballoon ablation was initiated.
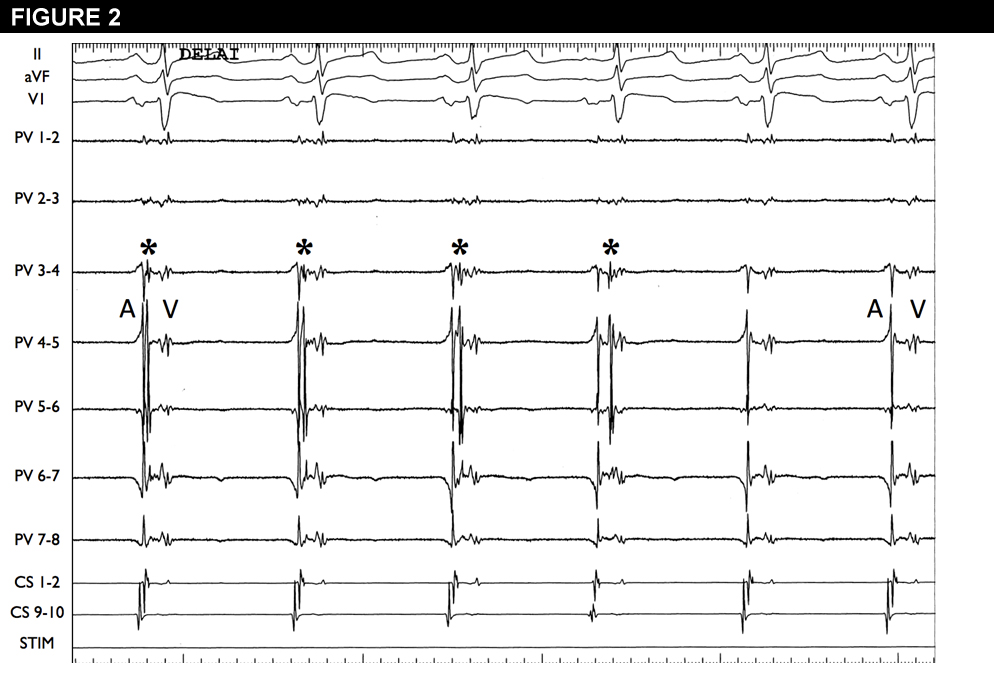
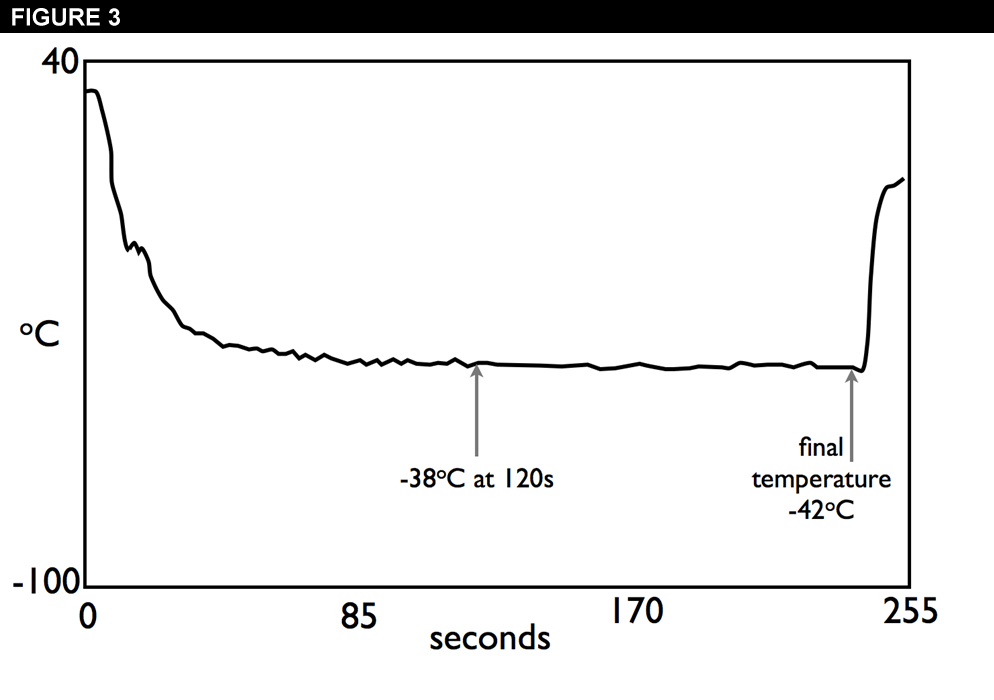
Approximately 90 seconds after the initiation of cryoballoon ablation a delay in left atrial-PV conduction was observed (*) followed by persistent LA-PV (entrance) conduction block (Figure 2). Cryoablation was continued for a standard four-minute cycle after which entrance and exit block was verified. Figure 3 demonstrates the cryoballoon temperature curve during the cryoballoon application.
With respect to this PV, what would you do next?
Show Answer
The correct answer is: C. Rewire the PV to reorient the CB prior to applying 1 further “bonus” cryoapplication.
Recently clinical and preclinical studies have demonstrated that cryothermal ablation using a balloon catheter provides an effective means to achieve lasting electrical isolation of the pulmonary veins.1 This case illustrates some of the unique aspects of the cryoballoon ablation (CBA) procedure.
First, while the pulmonary vein (PV) was undeniably isolated during the cryoapplication (Figure 2) careful examination of the ablation characteristics suggest that the likelihood of durable PVI with this cryoapplication is reduced. Given the importance of optimal circumferential tissue contact in the achievement of lasting PVI, it is standard practice to assess the adequacy of PV occlusion with the injection of contrast through the cryoballoon catheter's central lumen. In our case the patient had a small degree of contrast leak at the inferior aspect of the cryoballoon (CB) prior to the onset of cryoablation (Figure 1). In some cases the presence of a small degree of localized leak may be acceptable due to the potential for improved seal associated with the expansion of the cryoballoon's volume at the onset of ablation. However, should the leak persist, then the convective heating of the CB by the intervening blood will reduce the efficiency of freezing and the durability of the lesion.
As such, when a small leak is observed with pre-ablation contrast injection, it is important to carefully monitor the characteristics of the cryoapplication. Specifically, independent prognostic information regarding the efficacy of the ablation lesion can be derived from observation of the cryoballoon temperature achieved during ablation, as well as the time to PVI as assessed by the Achieve CMC. In terms of CB temperature, studies have demonstrated that a minimal cryoballoon temperature at the end of freezing colder than -51°C can predict PVI with 100% specificity for both superior and inferior PVs. In contrast, a cryoballoon temperature at 120 seconds warmer than -36°C for superior PVs and -33 °C for inferior PVs can predict ineffective PVI with 95% specificity (PPV 80%) and a 97% specificity (PPV 82%) respectively.2 Similarly, a recent study demonstrated that sustained PVI was associated with a shorter mean time to conduction block (39 seconds) when compared to PVs with recovered PV conduction (125 seconds).3 The authors identified a cut-off time of 83 seconds for the prediction of stable sustained PVI without reconduction (86% sensitivity and 97% specificity). In our case, the relatively warm nadir temperature (-42oC) and relatively prolonged "time to isolation" (90 seconds) suggest that the lesion may have been compromised, and despite the attainment of acute PVI additional ablation is required.
Additionally, even in the presence of an ideal cryoapplication there is evidence supporting the use of a repeated freeze–thaw cycle. Since the early days of cryosurgery there has been a recognition that repeated freeze–thaw cycles produce faster and more extensive tissue cooling, which will extend the lethal effect of the ablation lesion to the outer limit of the frozen volume (i.e. the warmer freezing temperature zone at the periphery of the target tissue). Thus, even in the event of an optimal ablation lesion, most clinicians will opt to deliver a bonus application on spec.
As such, when the above is taken into account, observation (Option A) is likely inappropriate. By extension, and in consideration of the lack of additional prognostic information provided by adenosine and/or isoproterenol testing in patients undergoing CBA, provocation testing (Option B) is also inappropriate.4-6
Therefore, the question becomes the means to which further ablation will be provided: (1) immediate reablation with the CB (Option D), vs. (2) repositioning the CB prior to reablation (Option C). The deciding factor between these two options can be derived from an understanding of cryoballoon catheter anatomy. The current generation CB catheter realizes an ablation lesion via the delivery of pressurized cryorefrigerant (nitrous oxide; N2O) to the distal aspect of the inner balloon through an ultrafine injection tube. Thereafter, the refrigerant is sprayed to the distal face of the balloon through 4 jets positioned slightly distal to the cryoballoon equator at 90° from one another. This results in a large circular zone of cooling extending from the proximal aspect of the CB equator to a few mm towards its distal face. It is important to note that in the first generation CB there is a slight heterogeneity in the cooling temperature within the zone of optimal cooling. Specifically, the ablation temperature in the regions between consecutive refrigerant jets is relatively warmer than in the areas directly opposing the jets. Thus, even with optimal tissue contact within the zone of optimal cooling there exists the potential for a regional reduction in freezing efficiency. As such step-wise ablation using the combination of axial catheter rotation, catheter flexion, and/or repositioning of the guidewire within a different distal PV branch in order to reorient the balloon's axis will ensure that the entire circumferential surface of the PV ostium is adequately ablated. Of note, it is possible that the second generation will overcome these limitations through an update to the N2O refrigerant distribution system that allows for more homogeneous cooling in a wider refrigerant band.7
Lastly, it should be noted that a recent prospective study demonstrated no benefit, and potential harm, with the performance of multiple (2) bonus lesions when compared to a single "insurance" cryoapplication.8
References
Andrade JG, Khairy P, Guerra PG, et al. Efficacy and safety of cryoballoon ablation for atrial fibrillation: A systematic review of published studies. Heart Rhythm 2011;8:1444-1451.
Furnkranz A, Koster I, Chun KR, et al. Cryoballoon temperature predicts acute pulmonary vein isolation. Heart Rhythm 2011;8:821-825.
Dorwarth U, Schmidt M, Wankerl M, Krieg J, Straube F, Hoffmann E. Pulmonary vein electrophysiology during cryoballoon ablation as a predictor for procedural success. J Interv Card Electrophysiol 2011;32(3):205-11.
Chierchia GB, Yazaki Y, Sorgente A, et al. Transient atriovenous reconnection induced by adenosine after successful pulmonary vein isolation with the cryothermal energy balloon. Europace 2009;11:1606-1611.
Jiang CY, Jiang RH, Matsuo S, et al. Early detection of pulmonary vein reconnection after isolation in patients with paroxysmal atrial fibrillation: a comparison of ATP-induction and reassessment at 30 minutes postisolation. J Cardiovasc Electrophysiol 2009;20:1382-1387.
Chun KR, Furnkranz A, Metzner A, et al. Cryoballoon pulmonary vein isolation with real-time recordings from the pulmonary veins. J Cardiovasc Electrophysiol 2009;20:1203-1210.
Andrade JG, Dubuc M, Guerra PG, et al. The Biophysics and Biomechanics of Cryoballoon Ablation. Pacing Clin Electrophysiol 2012; doi: 10.1111/j.1540-8159.2012.03436.x. [Epub ahead of print].
Chun KR, Furnkranz A, Koster I, et al. Two Versus One Repeat Freeze-Thaw Cycle(s) After Cryoballoon Pulmonary Vein Isolation: The ALSTER EXTRA Pilot Study. J Cardiovasc Electrophysiol 2012; doi: 10.1111/j.1540-8167.2012.02315.x. [Epub ahead of print].