A 64-year-old gentleman with past medical history significant for dilated, ischemic heart disease with an ejection fraction of 20%, Stage D, NYHA IV and remote coronary artery bypass surgery presents with intermittent, symptomatic hypotension two weeks following an uncomplicated left ventricular assist device (LVAD) implantation for destination therapy. Vital signs at baseline demonstrated a mean arterial pressure (MAP) by Doppler of 70-80mmHg, HR 70s, 92% pulse oximetry on room air, and stable pulsatility index (PI) 4-6. Findings on physical exam were remarkable for non-focal neurologic exam, elevated JVP, LVAD hum, and 2-3 plus lower extremity pitting edema. EKG was significant for chronic atrial fibrillation and ventricular paced rhythm at 70bpm. Chest x-ray showed cardiomegaly, trace bilateral pleural effusions, LVAD, and CRT-D device. Laboratory values were significant for stable hemoglobin at 8.7g/dL, normal electrolytes, Cr 0.8mg/dL, total bilirubin 2.8mg/dL, INR 1.4, and an LDH of 426 U/L (mildly elevated). While on the regular nursing floor patient intermittently developed altered mental status in the setting of PI alarms, which correlated with a drop in MAP by Doppler to 40-50mmHg. There was no evidence of LVAD power spikes and pump flows dropped with respect to fluctuations in PI. Symptoms rapidly resolved with IV fluid bolus.
What do you think is the most likely etiology of intermittent hypotension and PI events in this postoperative patient?
Show Answer
The correct answer is: D. Tamponade
Clinical presentation was concerning for tamponade and confirmed following a thorough diagnostic evaluation. An initial echocardiogram demonstrated a small posterior effusion, small left ventricle, and normal right ventricle without echocardiographic evidence of tamponade. However, quality was limited secondary to body habitus and acoustic shadowing from hardware. In the interim, patient was moved to the intensive care unit for further observation and invasive hemodynamic monitoring. Right heart catheterization demonstrated equalization of pressures: RA 14mmHg, PA 47/20(31), PCW 14mmHg and cardiac indices by thermodilution were 5.8/2.6. A CT scan with IV contrast (Figure 1) was subsequently obtained and confirmed clinical suspicion of tamponade. Patient underwent a left posterolateral thoracotomy for removal of dense clot. At one year follow-up patient continues to do well without subsequent episodes of tamponade.
Diagnosis of tamponade in a patient with a continuous flow LVAD can be difficult. Evidence of LVAD inflow obstruction may result in decrease pump flows and PI alarms. These events can be seen in both the setting of cardiac tamponade and hypovolemia.1 In a patient with a continuous flow LVAD, Beck's classic clinical findings may not hold true.2 To confirm diagnosis physicians should have a low threshold to obtain additional objective data points through echocardiogram, CT with IV contrast, and/or right heart catheterization.1, 3
Pump thrombosis is a potential LVAD complication, but less likely in this case given lack of hemolysis and absence of power surges.1, 4
Right heart failure is also a valid concern, but true right heart failure would not be intermittent and is not the best choice in this situation.
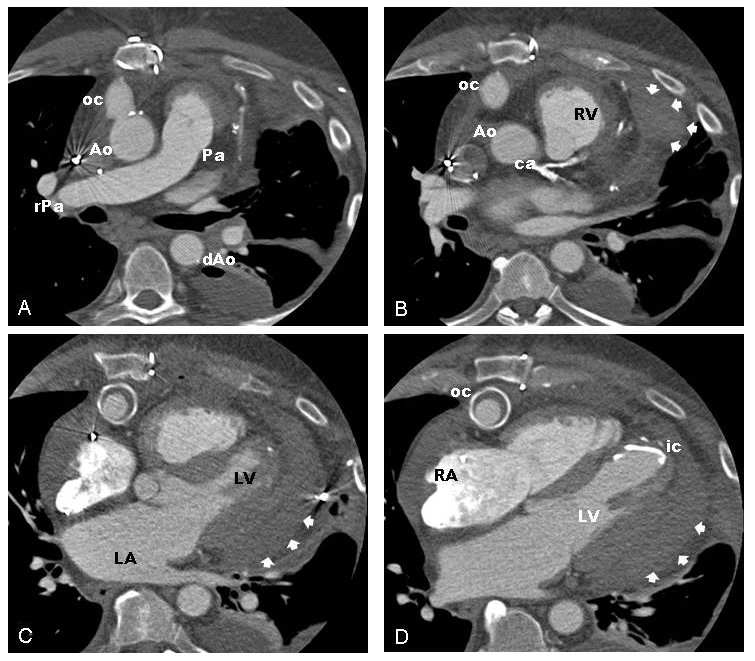
Figure 1
CT images from base to apex (A-D) depict posterior hemopericardium with extrinsic compression of left ventricle. Legend: Ao – aorta, ca – coronary artery, ic – LVAD inflow cannula (partial visualization), LA – left atrium, LV – left ventricle, Pa – pulmonary artery, oc – LVAD outflow cannula, rPa – right pulmonary artery, RA – right atrium, RV – right ventricle, and Arrows - pericardial effusion.
References
Slaughter, M.S., et al., Clinical management of continuous-flow left ventricular assist devices in advanced heart failure. J Heart Lung Transplant, 2010. 29(4 Suppl): p. S1-39.
Beck, C.S., Two Cardiac Compression Triads. JAMA, 1935. 104(9): p. 714-716.
Roy, C.L., et al., Does this patient with a pericardial effusion have cardiac tamponade? JAMA, 2007. 297(16): p. 1810-8.
INTERMACS Manual of Operations and Procedures, Version 4.0, Appendix A. 2014.