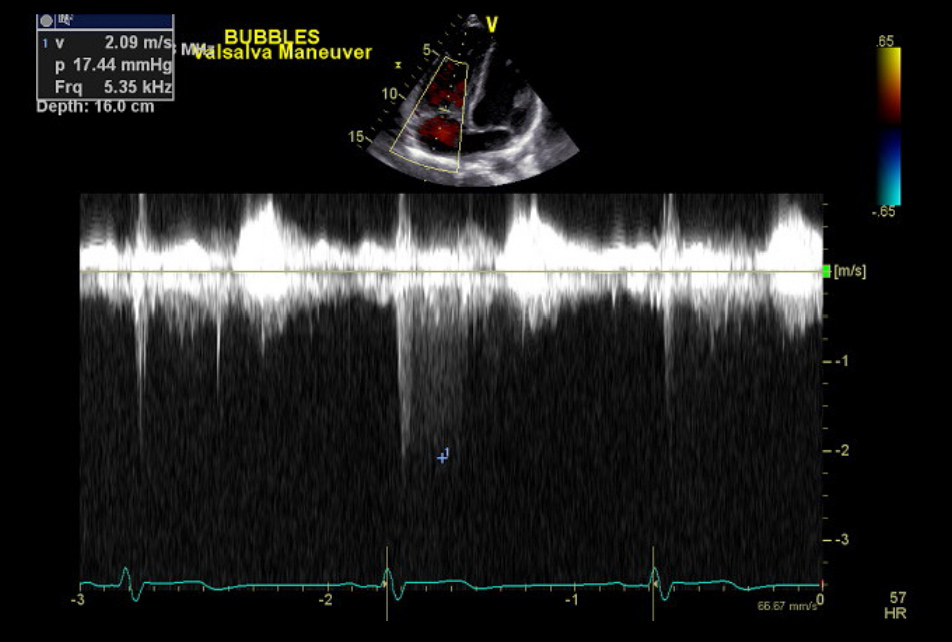
A 19-year-old male asymptomatic NCAA Division I tennis player presents to your clinic as a referral for an abnormal pre-participation screening ECG (Figure 1). The patient denies any history of chest pain, palpitations, syncope, or shortness of breath. The patient has never had problems keeping up with workouts, and generally considers himself one of the more fit players on the tennis team. He denies any family history of heart disease or sudden cardiac death. His exam is notable for a soft I/VI mid systolic murmur over the pulmonic area and a fixed-split S2. Based on these findings an echo is performed (Figure 2; Video 1, 2, 3, and 4).
Figure 1
Figure 2
Video 1
Video 2
Video 3
Video 4
Which of the following statements is true regarding further management in this patient's case?
Show Answer
The correct answer is: E. The patient can participate in all competitive sports.
Based on the case, physical exam, and imaging the patient has a secundum atrial septal defect (ASD) without evidence of pulmonary hypertension. His EKG is significant for right axis deviation and right ventricular hypertrophy (Figure 1). Echo images demonstrate mild right ventricular enlargement (Video 1) in an athlete whose sport requires a high dynamic component. His right ventricle (RV) could be enlarged based on the high level of training required at the collegiate level (RA size was normal). Further imaging revealed a secundum ASD (Video 2, 3). Given his lack of symptoms or evidence of pulmonary hypertension (Figure 2; Video 4), which demonstrates normal RV systolic pressure and lack of septal flattening, he should be cleared to play all competitive sports.
Option E is the correct answer based on the Bethesda guidelines for athletes with congenital heart defects. Specifically, patients with large ASD without symptoms or signs of pulmonary hypertension can participate in competitive sports without restriction. Patients with a large ASD and signs of mild pulmonary hypertension can participate in low-intensity competitive sports. Those with signs of more severe pulmonary hypertension, right to left shunt, or cyanosis, cannot participate in competitive sports.
Option A is an incorrect choice as he does not have signs of pulmonary hypertension and can therefore participate in any competitive sport.
Option B is an incorrect choice because sufficient evidence exists that there are certain findings, when found in isolation on ECG, which do not portend serious underlying cardiac disease. These "borderline" findings include left atrial enlargement, right atrial enlargement, right axis deviation, left axis deviation, right ventricular hypertrophy, and T-wave inversion in leads V1-V4 in people of African-Caribbean descent. However, if two or more of these "borderline" ECG findings are present, it should be considered abnormal and would warrant further testing.
Option C is an incorrect choice due to the fact that a sinus bradycardia is a common finding in well trained athletes. Furthermore, due to the high vagal tone found in athletes, other rhythm findings that are considered "normal" include: sinus bradycardia ≥30 bpm, sinus arrhythmia, junctional/nodal rhythms, 10 AV block, Mobitz Type-I 20 AV block, and ectopic atrial rhythms.
Option D is incorrect; based on the Bethesda guidelines the patient would have to wait three to six months prior to participation after surgical or percutaneous ASD closure.
References
Graham TP Jr, Driscoll DJ, Gersony WM, Newburger JW, Rocchini A, Towbin JA. Task Force 2: congenital heart disease. J Am Coll Cardiol 2005;45:1325-33.
Drezner JA, Ackerman MJ, Anderson JM, et al. Electrocardiographic interpretation in athletes: the 'Seattle Criteria.' Br J Sports Med 2013;47:122-4.
Riding NR, Sheikh N, Adamuz C, et al. Comparison of three current sets of electrocardiographic interpretation criteria for use in screening athletes. Heart 2015;101:384-90.
Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e143-e263.