A 35-year-old male was referred by his PCP with a history of a single episode of atrial fibrillation (AF) with a ventricular rate in the 160-170 range lasting over 24 hours, which had been documented before DCCV in an outside ER. In retrospect, he had noted similar short-lived and self-terminating symptoms on a few occasions in the past but with no clear patterns of occurrence. He had no other cardiovascular or respiratory complaints. He was active with no limitations. There were no symptoms suggestive of dysthyroidism and he was systemically well.
Figure 1
He had no past medical history. He was on no medications and had no allergies.
He was an outdoor activities instructor. He did not smoke, use alcohol or drugs.
Family history was notable for his paternal grandfather who had died of a heart attack at the age of 39. The patient's father had been diagnosed with hypertension but family history was otherwise unremarkable.
A comprehensive physical exam revealed no abnormalities.
Initial labs including TSH were normal.
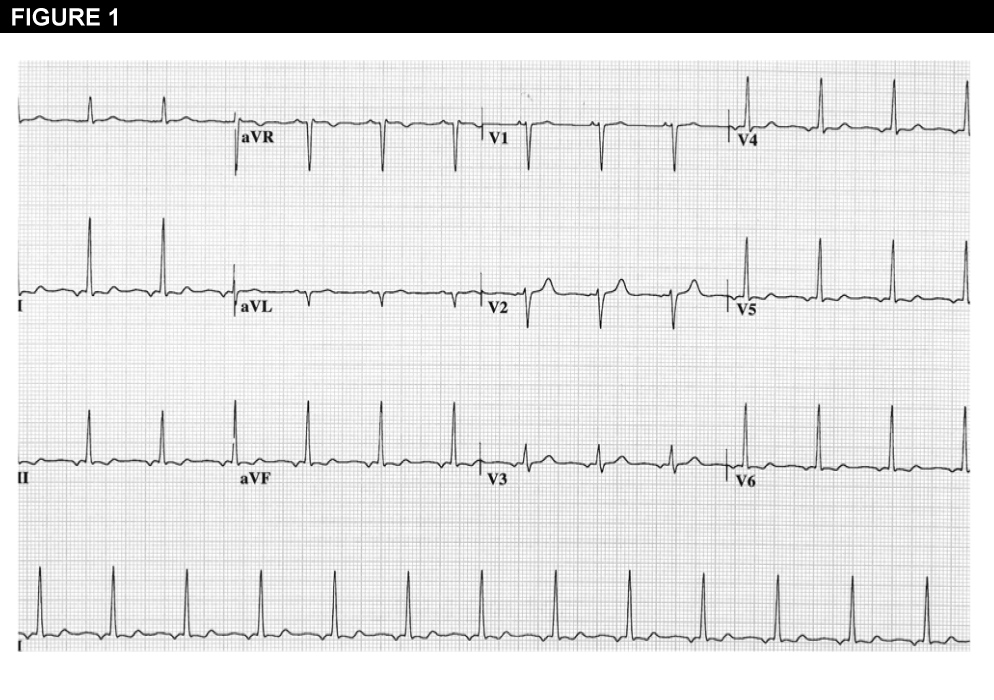
The 12-lead ECG obtained immediately after the DCCV revealed an ectopic atrial rhythm and some diffuse non-specific ST and T wave abnormalities (Figure 1), but a subsequent ECG was completely normal.
Echocardiogram was normal including LA dimensions.
An ETT had been performed at the outside ER prior to discharge. This was terminated at 12 minutes with a peak heart rate of 170/min, with no symptoms and no evidence of reversible ischemia or arrhythmia.
What other potential etiologies for the atrial fibrillation must be considered in this case?
Show Answer
The correct answer is: C. Familial cardiomyopathy
This young man presented with what had originally been framed as lone atrial fibrillation. However, there are several features of this case that raise the possibility of an underlying cardiomyopathy-despite the normal echo. On review of his initial 12-lead ECG, while post cardioversion ECG abnormalities are not uncommon, the nature and extent of these is somewhat more than one would typically encounter. In addition, the age of onset of his AF significantly increases the likelihood of an inherited form and this suggestion is only compounded by the history of premature sudden death in his paternal grandfather.1, 2
Occult hypertension is certainly possible and paroxysmal AF has been reported with phaeochromocytoma and other unusual causes of secondary hypertension, but there were no clinical features to suggest this. Pulmonary venous ectopy is a potential mechanism of AF in this individual, though its relationship to different forms of primary cardiomyopathy has not been systematically explored.3
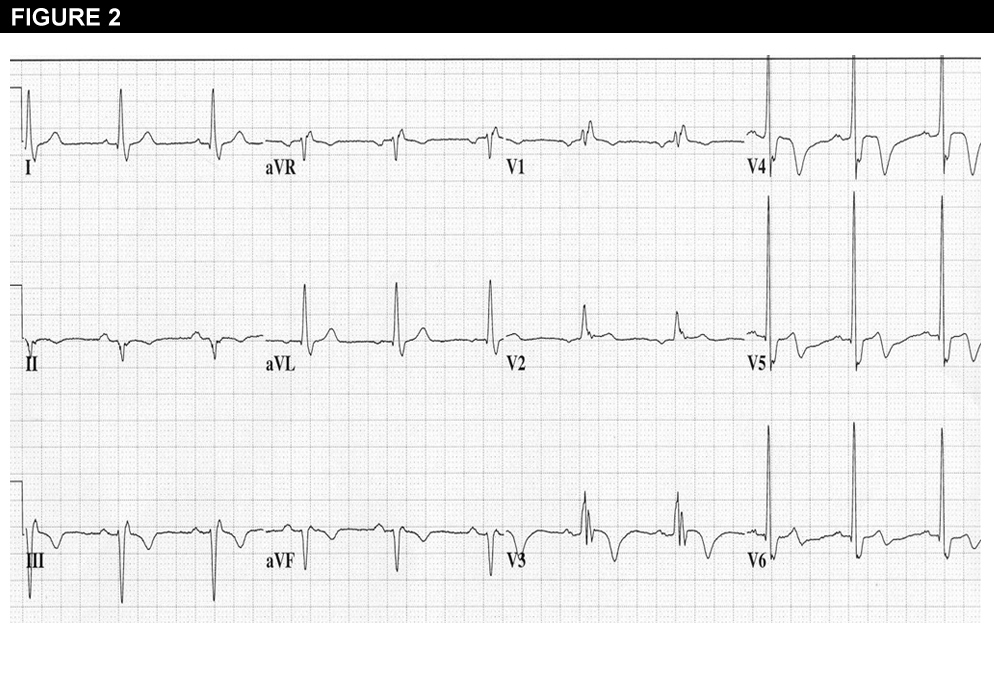
In this patient, a detailed family history was obtained and additional data were gleaned from family members. It transpired that the paternal grandfather had not had an ischemic prodrome or any acute chest pain but had died suddenly at the breakfast table.4 The patient's father had been diagnosed with essential hypertension, but on echocardiogram had 22mm concentric LVH and an ECG suggestive of HCM (Figure 2). Under these circumstances the patient was followed as a probable case of subclinical or preclinical HCM and it was recommended that all at risk family members be screened with ECG and Echo as per ACC/AHA guidelines.5
Two years later, his paternal uncle died suddenly at the age of 42 and an autopsy revealed LV noncompaction. At this stage an MRI of the patient documented eccentric LVH, some RVH and possible non-compaction (Full pedigree outlined in Figure 3). These data and the family history of two premature sudden deaths led to the implantation of an ICD.
The case illustrates several important features of atrial fibrillation, long recognized from the basic literature, but only recently reaching clinical practice. Sustained AF is remarkably difficult to achieve in any animal model without some ongoing stimulus (e.g. pacing) and when the stimulus is removed there is rapid reversion to normal sinus rhythm.6 These data suggest that the atrium that is prone to persistent fibrillation is intrinsically abnormal and subsequent human genetic studies have supported a strong inherited predisposition to AF in many different settings including lone AF. Systematic studies have identified some forms of AF that behave as autosomal dominant conditions with reduced penetrance1, and there are also common genetic variants that increase the risk of AF or atrial flutter by as much as 3-4 fold.7 Epidemiologic studies where AF and CHF are each substantive risk factors for the other likely reflect in part a shared underlying mechanism in a subset of these syndromes.8
In parallel, long term studies of extended families with inherited forms of heart muscle disease have recognized that AF is a cardiomyopathy equivalent in at risk individuals. For most prevalent cardiomyopathies, first-degree relatives have a priori a 50% chance of having inherited the mutant copy of the gene. Lone AF has been reported as an initial manifestation of HCM, DCM, ARVC and diverse generalized myopathies including muscular dystrophy and myotonic dystrophy.9 As a result almost any cardiac abnormality in a young 'at risk' family member is much more likely to be a manifestation of such cardiomyopathy than an incidental finding. Age-related penetrance and pleiotropy are both recognized confounders and many family members have much less classic clinical features than the traditional index cases or probands.4 In older family members while acquired causes become more likely, they remain less likely than the cardiomyopathy segregating through the family.
Together these observations argue for a rigorous family history in cases of AF and consideration of potential inherited causes of the arrhythmia especially in the setting of early onset where the etiology is not clear. To date there is no clear role for genetic testing in AF, but the field is changing rapidly. Challenging families are best referred to centers with expertise in inherited heart disease. While these efforts may not lead to any immediate changes in the management of the AF, they are quite likely to change the overall management of the patient and the patient's family over time.
References
Ellinor PT, Yoerger DM, Ruskin JN, MacRae CA. Familial aggregation in lone atrial fibrillation. Hum Genet 2005;118:179-84.
Arad M, Seidman JG, Seidman CE. Phenotypic diversity in hypertrophic cardiomyopathy. Hum Mol Genet 2002;11:2499-506.
Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659-66.
Sen-Chowdhry S, Jacoby D, McKenna WJ. The implications of inheritance for clinical management. Circ Cardiovasc Genet 2012;5:467-76.
Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, et al. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol 2003;42:1687-713.
Sinner MF, Ellinor PT, Meitinger T, Benjamin EJ, Kaab S. Genome-wide association studies of atrial fibrillation: past, present, and future. Cardiovasc Res 2011;89:701-9.
Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation 2003;107:2920-5.
Sabeh MK, Macrae CA. The genetics of atrial fibrillation. Curr Opin Cardiol 2010;25:186-91.