A 66-year-old man with five prior atrial fibrillation (AF) ablations was referred for electrophysiological evaluation following recurrent supraventricular tachycardia resulting in tachycardia-induced cardiomyopathy with an ejection fraction of 38%. After dofetilide failure, amiodarone suppressed the tachycardia, and his ejection fraction recovered to 60%. He discontinued amiodarone, fearing long-term side effects. An electrophysiological study was performed, and an atrial tachycardia with two distinct, alternating cycle lengths was easily induced with burst pacing (Figure 1). Attempted entrainment at one location in the left atrium is shown (Figure 2). Ablation at this location resulted in the tachycardia cycle length becoming fixed, and then the tachycardia terminated (Figure 3).
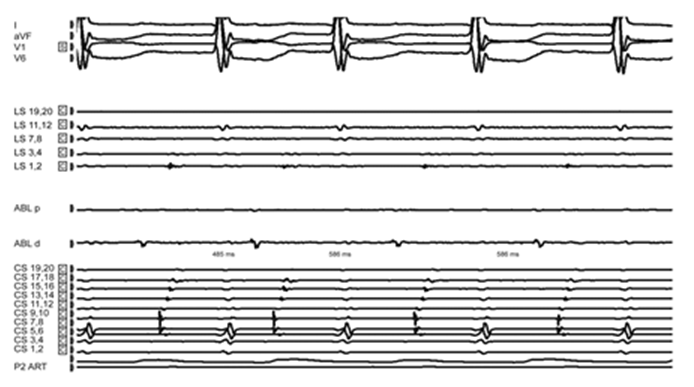
Figure 1
Atrial burst pacing induced a reproducible tachycardia with a cycle length fluctuating between 485 and 586 ms. ABL d = distal ablation catheter; ABL p = proximal ablation catheter; CS = coronary sinus catheter; LS = left atrial halo catheter (alternate electrogram pairs are shown because, other than LS 1, 2, all other left atrial halocatheter electrode pairs did not record any discernible electrogram).
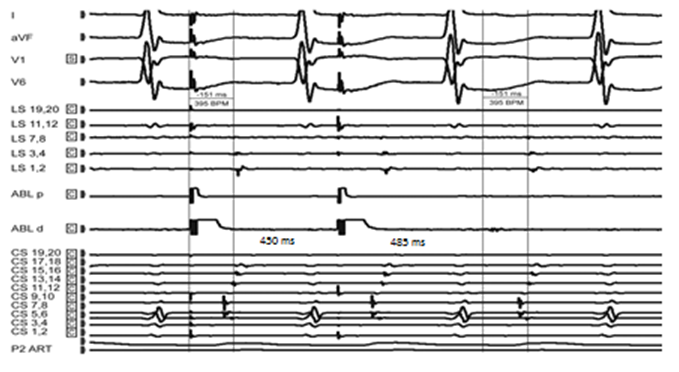
Figure 2
Attempted entrainment from the mapping catheter in the left atrium. As the surface P was diminutive, the time interval from stimulus (ablation distal pair electrodes) to LS 3,4 electrodes was measured. This is equal to the interval between the ablation distal electrogram to LS 3,4 electrogram during tachycardia. Post pacing interval while pacing at 450 ms was equal to the shorter of the two tachycardia cycle lengths (485 ms).
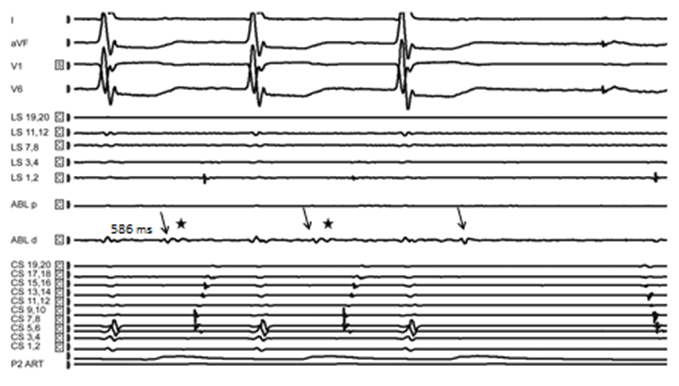
Figure 3
Termination of the tachycardia during ablation at the point of attempted entrainment. Note that the block occurred in the centralisthmus between the high-frequency component (solid arrow) and the low-frequency component (star) of the multicomponent fractionated electrogram.
Which of the following statements describes the mechanism of tachycardia?
Show Answer
The correct answer is: C. Reentry with two different paths within critical isthmus.
Atrial fibrillation ablation has become a frequently performed procedure since ectopic sources, particularly those in the pulmonary veins, were found to produce AF.1 Although maintaining sinus rhythm is the goal of the procedure, atrial tachyarrhythmia occur after AF ablation and include recurrent atrial fibrillation, atypical atrial flutter and reentrant and nonreentrant focal atrial tachycardia.2,3
The cumulative effect of multiple prior ablations is a large area of atrial myocardium with low-voltage electrograms (<0.05 mV). Low-voltage electrograms make electroanatomic mapping difficult because a substantial portion of the left atrium appear unmapped.
However, the attempted entrainment of the tachycardia in this patient suggested a likely mechanism.
Overdrive suppression did not occur on repeated attempts at shorter cycle lengths, making it unlikely that automaticity was the principal mechanism.
Similarly, pacing did not result in acceleration of the tachycardia, indicating that triggered activity is unlikely.
Interpretation of entrainment in a tachycardia with fluctuating cycle length requires the careful use of all measurable entrainment criteria with reasonable substitution if necessary.
Diminutive surface "P" waves significantly increase the challenge of recognizing concealed versus manifest entrainment.
Intracardiac electrogram may be used as a surrogate to distinguish concealed from manifest entrainment by demonstrating fusion. The reliability of this observation is improved with a higher number of intracardiac electrodes.
Variable fusion occurring at different pacing cycle lengths on the available intracardiac electrograms indicates reentry rather than another mechanism. In tachycardia with fluctuating cycle lengths, if the post-pacing interval consistently matches one of the several original cycle lengths (usually the shorter cycle length) after multiple repetitions, the consistency of those post-pacing intervals also supports reentry.
The identical atrial activation sequence of the recorded electrograms of both cycle lengths of the tachycardia suggests that the difference in cycle lengths is attributable to the protected zone within the central isthmus. Two different paths with differential conduction/ repolarization properties within the central isthmus likely cause the two different cycle lengths.
In this patient, time measured from stimulus (pacing from the distal ablation electrodes) to a particular location of intracardiac electrogram was equal to time taken between the same electrodes during tachycardia. The post-pacing interval at this site was equal to the tachycardia cycle length and intracardiac electrograms during pacing suggested concealed fusion. The ratio of pacing site to surface P interval to tachycardia cycle length (shorter cycle length) could not be reliably assessed due to low amplitude P waves.
Radiofrequency ablation at this site changed the cycle length of the tachycardia to a fixed cycle length (elimination of the path with the shorter cycle length) prior to the termination of the tachycardia (block of the path with the longer cycle length). Spatial separation between the two paths is very minimal as the second ablation is adjacent to prior lesion. This patient has been arrhythmia free for over than a year based on symptoms and pacemaker electrogram assessment.
Atypical atrial flutter is a challenging clinical arrhythmia, and when it has fluctuating cycle lengths with diminutive surface P wave, several surrogate measures using intracardiac electrogram may aid in successful ablation.
References
Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659-66.
Ouyang F, Tilz R, Chun J, et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation. Circulation 2010;122:2368-77.
Gerstenfeld EP, Callans DJ, Sauer W, Jacobson J, Marchlinski FE. Reentrant and
nonreentrant focal left atrial tachycardias occur after pulmonary vein isolation. Heart Rhythm 2005;2:1195-1202.