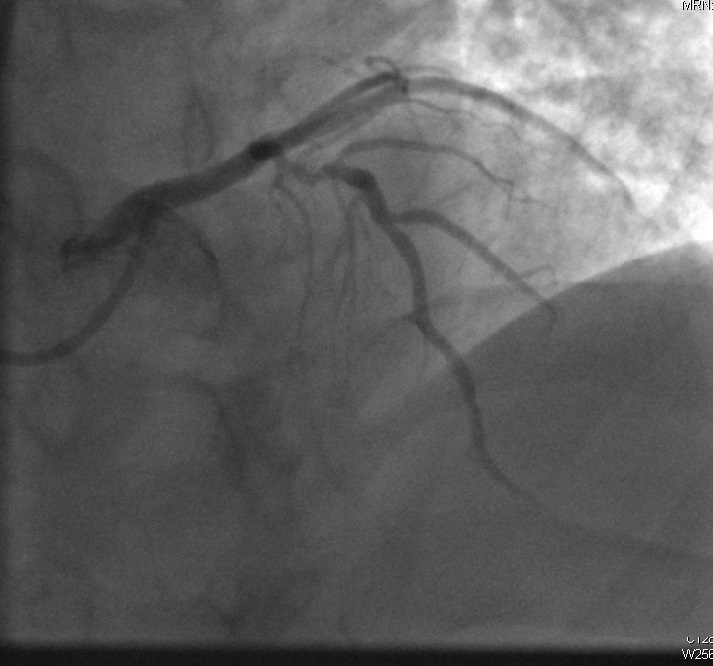
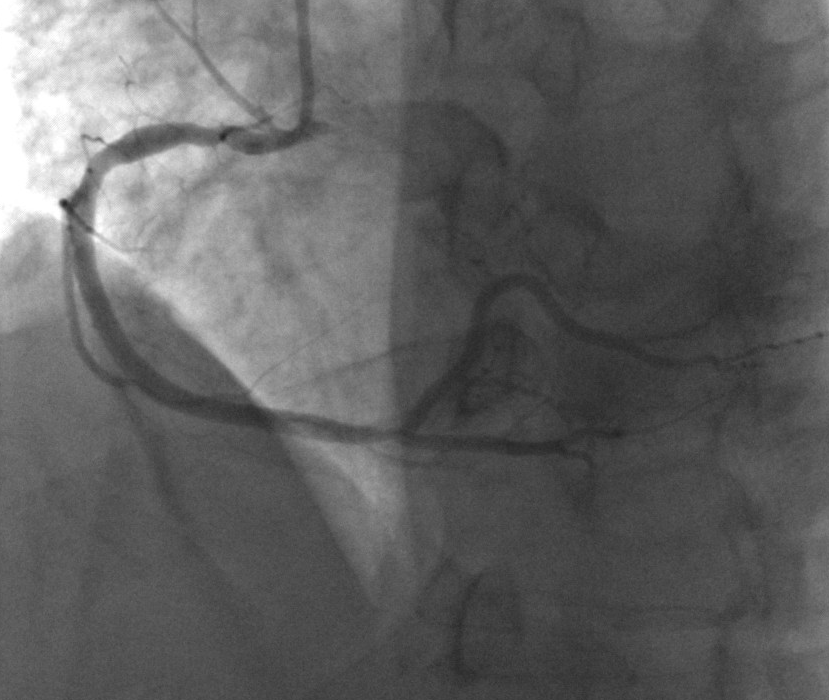
A 57-year-old man with a past medical history of hypertension and dyslipidemia presented to the cardiology clinic with a 1-year history of exertional retrosternal oppressive chest pain. The pain was stable over this period of time. The cardiac examination was unremarkable. An electrocardiogram showed normal sinus rhythm without ST or T segment changes. The transthoracic echocardiography showed normal left ventricular function without segmental wall abnormality or valvulopathy. Coronary computed tomography angiography showed high calcium score with calcified lesions in the left anterior descending (LAD) artery. He subsequently underwent angiography that revealed a 60% stenosis in the mid LAD with a fractional flow reserve of 0.96 (Image 1) and a non-stenotic right coronary artery (RCA) lesion with luminal narrowing <50% (Image 2). Based on the obtained result, the patient was diagnosed with chronic stable angina, and the decision was made to treat the patient medically.
Image 1
Image 2
Which of the following statements describes the benefit that could be derived from assessing the nonculprit RCA lesion with near-infrared (NIR) spectroscopy?
Show Answer
The correct answer is: B. NIR spectroscopy has long-term prognostic value with respect to the occurrence of major adverse cardiac events.
NIR spectroscopy can assess the lipid core burden index, which has been associated with cumulative major adverse cardiac events at 1 year. Imaging of the nonculprit coronary artery without significant stenosis allows assessment of the plaque composition with NIR spectroscopy.1
The obtained chromatograms provide two-dimensional information on cholesterol burden. IVUS, ocular coherence tomography, or NIR spectroscopy can be used to determine the presence of a thin-cap fibroatheroma.2 NIR spectroscopy specifically, compared with IVUS and ocular coherence tomography, has a higher ability to recognize monohydrate and ester cholesterol, which are abundant in necrotic areas and are key components of plaque vulnerability.
High lipid core burden index was found to be associated with worse overall prognosis. It remains to be determined whether the increased rate of major adverse cardiac events is related to the vulnerability of this specific lesion or to an increased risk throughout the entire coronary tree.
Although high-dose statin was found to decrease the lipid core burden index in obstructive lesions,3 studies that demonstrate a similar effect on nonobstructive lesions are still in process.
References
Oemrawsingh RM, Cheng JM, García-García HM, et al. Near-infrared spectroscopy predicts cardiovascular outcome in patients with coronary artery disease. J Am Coll Cardiol 2014;64:2510-8.
Kubo T, Akasaka T, Shite J, et al. OCT compared with IVUS in a coronary lesion assessment: the OPUS-CLASS study. JACC Cardiovasc Imaging 2013;6:1095-104.
Kini AS, Baber U, Kovacic JC, et al. Changes in plaque lipid content after short-term intensive versus standard statin therapy: the YELLOW trial (reduction in yellow plaque by aggressive lipid-lowering therapy). J Am Coll Cardiol 2013;62:21-9.