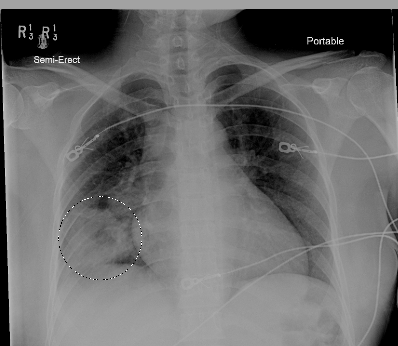
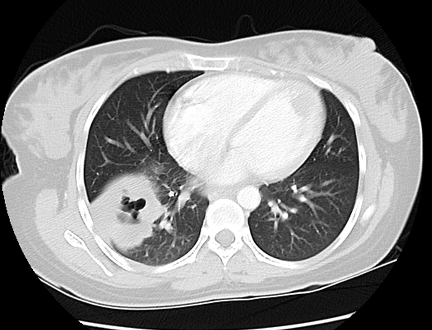
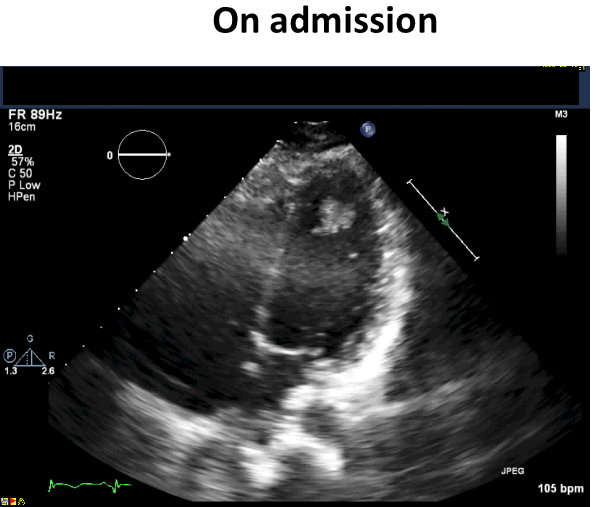
A 34-year-old previously healthy Hispanic woman presented to the emergency department with worsening left hip pain. Review of systems was significant for 15-pound weight loss, soaking night sweats, chills, and intermittent fevers over the past 3 months. On initial examination, she was hemodynamically stable and without focal clinical findings, with the exception of decreased breath sounds at the right base. Chest radiograph was significant for a large right lower lobe air space opacity (Figure 1). Computed tomography (CT) confirmed a cavitary lung mass; additional findings included a left ventricular (LV) filling defect consistent with an LV apical mass or thrombus (Figure 2), low density liver lesions, mediastinal lymphadenopathy, and a lytic left hip lesion highly concerning for metastatic neoplasm. Bronchoscopy and subcarinal lymph node biopsy demonstrated adenocarcinoma, which was presumed from a primary lung source. Transthoracic echocardiogram (TTE) (Figure 3) noted a spherical mass in the LV that appeared well-adherent to the apical aspect of the anterolateral wall in addition to an independently mobile echodensity adherent to this mass, which likely represented thrombus.
Figure 1: Chest Radiograph With Right Lower Lobe Airspace Opacity
Figure 2: CT Chest With Cavitary Right Lower Lobe Lesion and LV Filling Defect
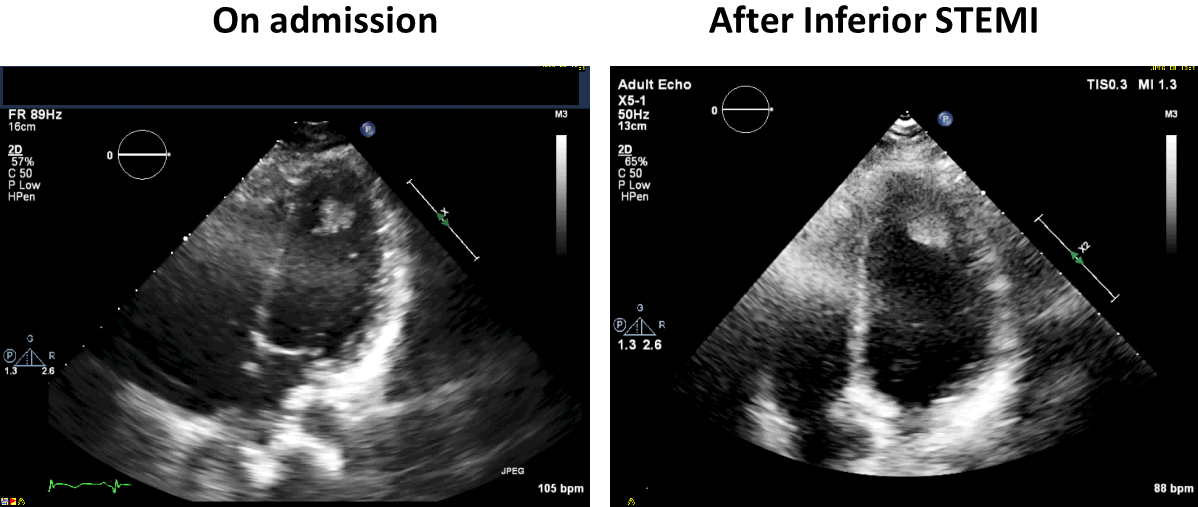
Figure 3: TTE With LV Mass With Adherent Mobile Echodensity
Mass appears to be at the apex but view is notably foreshortened.
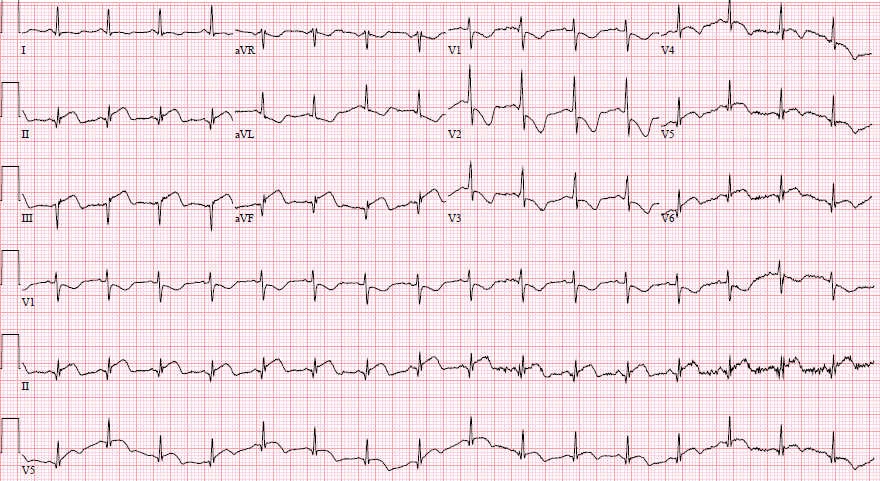
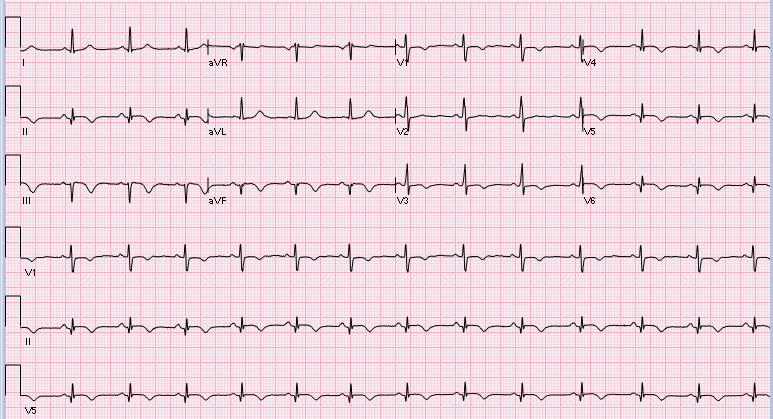
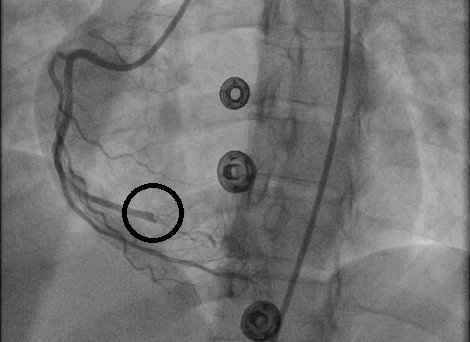
During a subsequent bone scan, she developed acute onset chest pain. Electrocardiogram (ECG) (Figure 4) demonstrated ST-segment elevations in leads II, III, and aVF consistent with ST-segment elevation myocardial infarction (STEMI). She was immediately taken to the cardiac catheterization laboratory where an acute occlusion was noted in the right coronary artery (RCA) (Figure 5) in the right posterolateral branch, right posterior descending artery, and the right marginal branch.
Figure 4: STEMI ECG
Comparison Initial ECG on Presentation
Figure 5: Coronary Angiography Preintervention
Based on the above coronary catheterization and clinical presentation, what is the likely etiology for the STEMI?
Show Answer
The correct answer is: C. Coronary embolism of thrombus or tumor
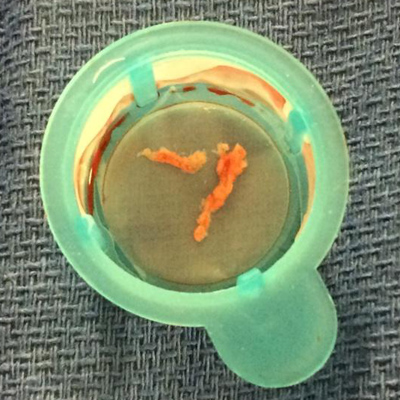
Given concern for coronary embolization, she received embolism aspiration, balloon angioplasty, and intracoronary eptifibatide with significant improvement in coronary flow (Figure 6). Pathology from the aspirated material showed organizing thrombus without evidence of tumor on cytology or staining (Figure 7). TTE showed stable LV systolic performance with inferior and posterior wall hypokinesis. Notably, the additional independently mobile echodensities adherent to the mass were no longer visualized on repeat echocardiogram (Figure 8). Subsequently, cardiac magnetic resonance imaging (CMRI) demonstrated a normal LV ejection fraction with inferoposterior hypokinesis and transmural delayed enhancement in the inferior-posterior wall consistent with prior infarction. Additionally, the CMRI demonstrated an LV mass adherent to the anterior LV wall, which took up contrast and appeared most consistent with tumor (Figure 9).
Figure 6: Coronary Angiography Postintervention
Figure 7: RCA Thrombectomy Specimen
Figure 8: TTE With LV Mass
No thrombus on repeat TTE after myocardial infarction.
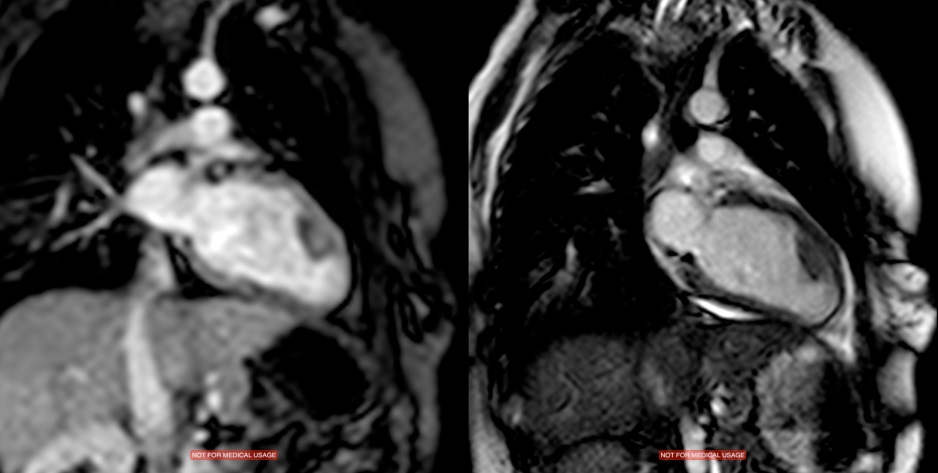
Figure 9: CMRI Two-Chamber View of Mass and Perfusion
Transmural delayed enhancement in the inferior-posterior wall. Notably, LV mass is adherent to the anterior LV wall, not the inferior-posterior defect consistent with history of RCA infarction.
Similar to primary cardiac tumors, cardiac metastases can present in myriad and protean ways that can mimic valvular heart disease, systolic heart failure, ventricular or supraventricular heart rhythm disturbances, conduction defects, syncope, embolism or pericardial effusion.1 Given this diagnostic difficulty, it should not be surprising that the frequency of cardiac metastases is generally underestimated, and, in fact, cardiac metastases are found in up to 25% of post-mortem patients who died of malignancies.2,3 According to one study, two thirds of all cardiac metastases involved the pericardium (69.4%), about one third involved the epicardium (34.2%) or myocardium (31.8%), and only 5% involved the endocardium.4 Endocardial invasion is rare and typically involves invasion of the left atrium from lung cancer or invasion of the right atrium from vena caval tumor.5,6,7,8 In one case series, 97 cases of lung cancer were associated with cardiac metastases, of which 0% and 24.6% had endocardial and myocardial metastases, respectively.4 As such, there are few case reports of metastases to the LV endocardium.9 One case report noted ventricular thrombi leading to cerebral embolism and other complications including complete atrioventricular block and LV outflow tract obstruction.10
Additionally, there have been some case reports of malignant coronary embolism from intracardiac metastases.11,12,13,14,15 A literature review found lung carcinoma to be the most common source (11/17 cases) for malignant coronary embolism and seemed to predominantly target the left circulation, with 8 embolisms in the left anterior descending artery, 5 in the left circumflex, 3 in the RCA, and 2 in the left main coronary artery.9
Here we present the case of an unfortunate young woman with widely metastatic lung adenocarcinoma including presumed metastasis to the anterior wall of the LV. The intracardiac metastasis was associated with intraventricular thrombus that seemingly caused STEMI by embolism down the right coronary distribution and was acutely treated with aspiration thrombectomy.
References
Reynen K, Köckeritz U, Strasser RH. Metastases to the heart. Ann Oncol 2004:15:375-81.
Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med 1993;117:1027-31.
Butany J, Leong SW, Carmichael K, Komeda M. A 30-year analysis of cardiac neoplasms at autopsy. Can J Cardiol 2005;21:675-80.
Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol 2007;60:27-34.
McLaughlin AM, Meaney JF, Keane J, O'Donnell RA. Left atrial invasion by pulmonary adenocarcinoma. Eur J Cardiothorac Surg 2007;31:936.
Ma Q, Liu D, Liu P, Chen J, Xie Z, D'Amico TA. Extensive invasion of the left atrium by lung cancer. Ann Thorac Surg 2013;96:685-7
Shimizu J, Ikeda C, Arano Y, et al. Advanced lung cancer invading the left atrium, treated with pneumonectomy combined with left atrium resection under cardiopulmonary bypass. Ann Thorac Cardiovasc Surg 2010;16:286-90.
Funakoshi Y, Mukohara T, Kataoka T, et al. Left atrial extension of metastatic lung tumor via pulmonary vein: report on the first case of Ewing sarcoma. Rare Tumors 2010;2:e53.
Son JW, Hong GR. Unusual left ventricular endocardial metastasis from primary lung cancer. J Cardiovasc Ultrasound 2012;20:157-60.
Kasai T, Kishi K, Kawabata M, Narui K, Momomura S, Yoshimura K. Cardiac metastasis from lung adenocarcinoma causing atrioventricular block and left ventricular outflow tract obstruction. Chest 2007;131:1569-72.
Kumagai N, Miura S, Toyoshima H, et al. Acute myocardial infarction due to malignant neoplastic coronary embolus. J Cardiol Cases 2010;2e123-e127.
Ackermann DM, Hyma BA, Edwards WD. Malignant neoplastic emboli to the coronary arteries: report of two cases and review of the literature. Hum Pathol 1987;18:955-9.
Karlsberg RP, Sagel SS, Ferguson TB. Myocardial infarction due to tumor embolism following pulmonary resection. Chest 1978;74:582-4.
Culver RA, Bampton PA, Bignold LP. Aortic and coronary embolism of anaplastic small-cell carcinoma of the lung. Med J Aust 1987;147:455-6.
Diaz Castro O, Bueno H, Nebreda LA. Acute myocardial infarction caused by paradoxical tumorous embolism as a manifestation of hepatocarcinoma. Heart 2004;90:e29.