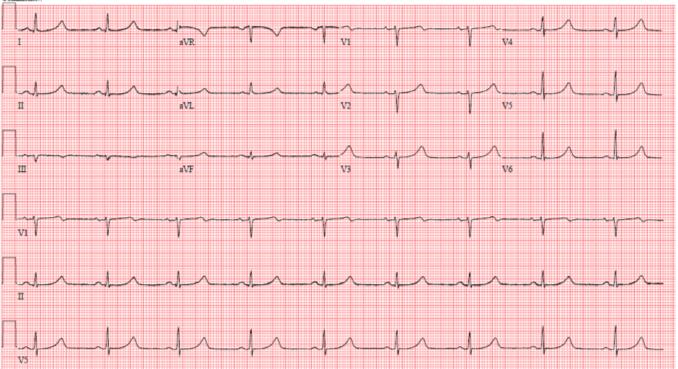
A young female patient presents to establish care in a cardiology clinic for further evaluation after surviving an out-of-hospital arrest. The patient began to experience fainting episodes at the age of seven and suffered an out-of-hospital cardiac arrest at the age of 12 while playing volleyball. A transthoracic echocardiogram demonstrated a structurally normal heart. Stress testing and coronary angiography were not performed. She has no other significant past medical history and is on no medications. The patient’s family history is notable for two distant relatives, nieces of her maternal-paternal great grandfather (her maternal grandmother's father), who died suddenly at young ages. The electrocardiogram (ECG) (Figure 1) was obtained from the patient.
Figure 1: Presenting ECG
Given the clinical history and characteristic findings in the ECG, which of the following is the next best step for this patient?
Show Answer
The correct answer is: C. Initiation of beta-blocker.
Long QT syndrome (LQTS) is an inherited disorder in which affected individuals have delayed ventricular repolarization manifest on surface ECG as QT prolongation. In most cases of LQTS, this repolarization abnormality is due to a decrease in one of two repolarizing potassium currents (LQT1, IKs; or LQT2, IKr) or an inappropriate increase in late sodium currents (LQT3, INa). The genes responsible for LQT1, LQT2 and LQT3 are KCNQ1, KCHN2 and SCN5A, respectively. The patient underwent genetic testing and was found to have L353P-KCNQ1, a previously reported mutation in LQT1.
Her presentation, suffering an arrest while exercising, and her ECG with symmetric, relatively normal T-waves with a QTc of 504 are prototypical for LQT1. Gene-specific triggers for cardiac events have been described in LQTS. Schwartz and colleagues identified 670 LQTS patients with known genotype who had cardiac symptoms (syncope, cardiac arrest, sudden death) and examined whether three specific triggers (exercise, emotion, sleep or rest without arousal) differed according to genotype. LQT1 is very distinctive, with 62% of events occurring during exercise and only 3% occurring during sleep/rest. The most common trigger in LQT2 is emotion, and sleep/rest is the most common trigger in LQT3. Zhang et al. described the ST-T-wave patterns in LQTS. The authors found four distinct patterns in LQT1, four patterns in LQT2 and two patterns in LQT3. In general, characteristic T-waves of LQT1 are broad-based and symmetric to relatively normal appearing; those in LQT2 are often bifid; and late-onset peaked/biphasic or asymmetric T-waves are found in LQT3.
According to the Heart Rhythm Society (HRS)/European Heart Rhythm Association (EHRA)/Asia Pacific Heart Rhythm Society (APHRS) consensus document regarding the diagnosis and management of inherited primary arrhythmia syndromes, the therapy for LQTS consists of initiation of beta-blockers for all symptomatic LQTS patients or asymptomatic patients with QTc ≥470 ms, ICD implantation for patients who survive cardiac arrest, avoidance of QT-prolonging drugs, identification and correction of electrolyte abnormalities, and referral to clinical expert for evaluation of risk prior to engaging in competitive sports. However, complications are not infrequent with ICD implantation, especially in young patients. Additionally, LQT1 patients typically have good responses to beta-blockers. In their study, Schwartz et al. found that 81% of LQT1 patients treated with beta-blocker were free of recurrences. The authors found the success rate of beta-blocker therapy was lower among LQT2 and LQT3 patients. Therefore, LQT1 patients who experience a cardiac arrest while not receiving beta-blocker may be treated with beta-blocker alone if there is a high risk associated with ICD implantation. Given this patient’s age, ICD implantation carries a high risk of morbidity over time. Consequently, initiation of beta-blocker alone is appropriate.
References:
Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol 2008;51:2291-2300.
Moss AJ, Shimizu W, Wilde AM, et al. Clinical aspects of type-1 long-QT syndrome by location, coding type, and biophysical function of mutations involving KCNQ1 gene. Circulation 2007;115:2481-9.
Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm 2013;10:1932-63.
Schwartz PJ, Prior SB, Spazzolini C, et al. Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias. Circulation 2001;103:89-95.
Zhang L, Timothy KW, Vincent M, et al. Spectrum of ST-T-wave patterns and repolarization parameters in congenital long-QT syndrome: ECG findings identify genotypes. Circulation 2000; 102:2849-55.