A 51-year-old male with familial dilated cardiomyopathy had his first heart transplant in 1990 and required a second heart transplant in 2003 because of graft vascular disease.
Since that the second transplant, follow-up was uneventful. Immunosuppression with triple therapy is established (cyclosporine A, mycophenolate mofetil, and steroids). Secondary to the calcineurin inhibitor treatment, he developed renal failure requiring a switch from cyclosporine to m-Tor inhibitors (baseline creatinine level 1.8 mg/dl and MDRD 42 mL/min/1.73 m2). In 2010, he had his first admission for heart failure (HF); suspecting cardiac rejection, a biopsy was performed confirming a Grade 1 acute rejection (Figures 1 and 2), which was treated conservatively (high-dose intravenous methylprednisolone).
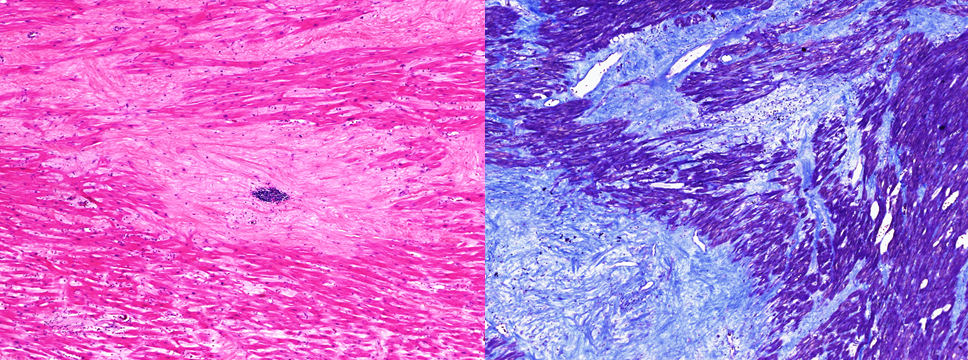
Figure 1
Left: Hematoxylin and eosin stain showing a significant interstitial infiltration of collagenous fibers betwenn myocites. Right: Masson trichrome stain confirming high density of collagenous fibers.
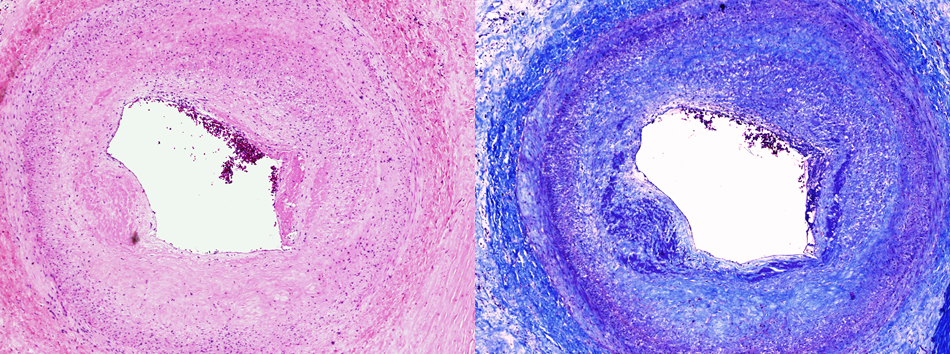
Figure 2
Left: Hematoxylin and eosin stain showing a coronary vessel wall thickening. Right: Masson trichrome stain of a coronary vessel.
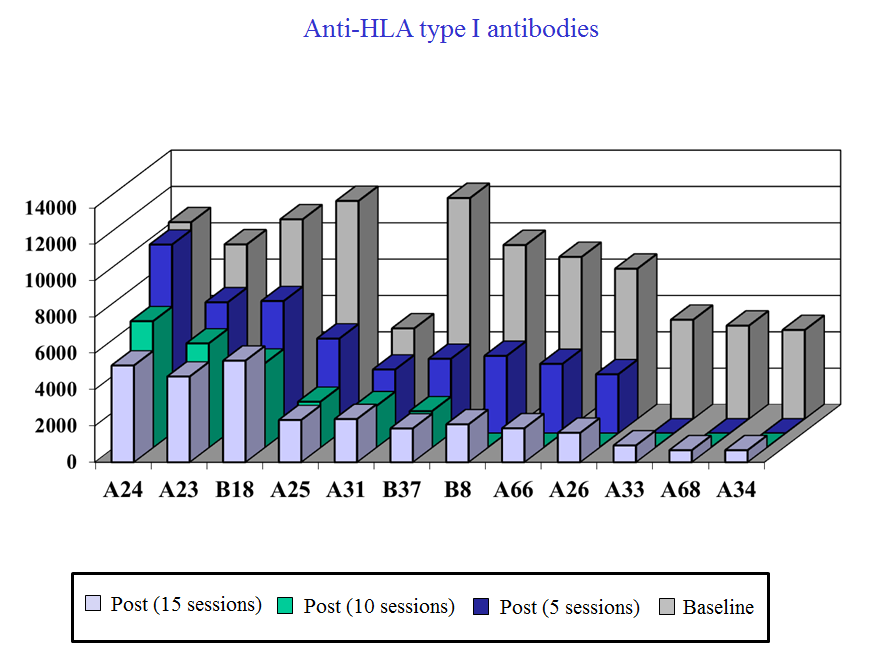
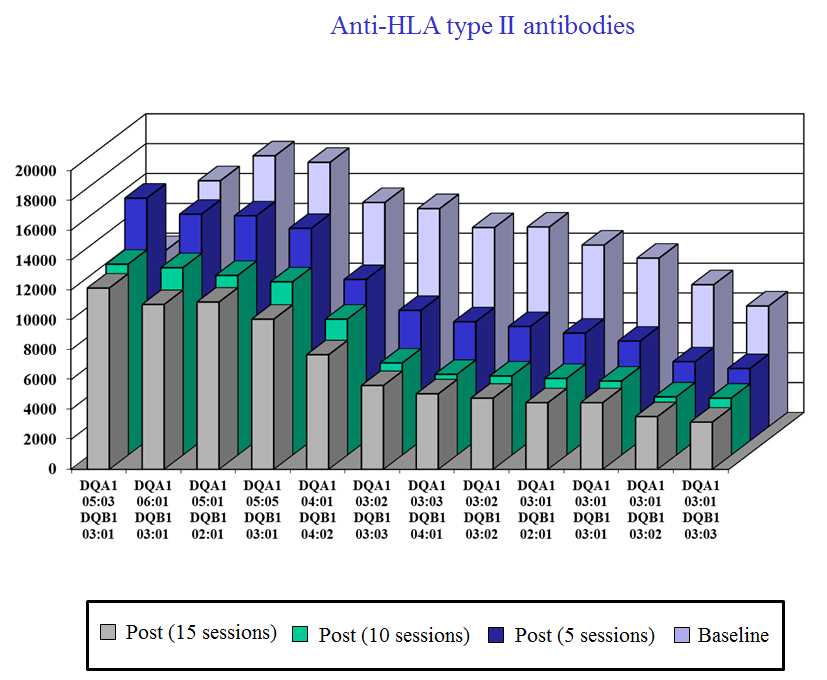
In one of his follow-up echocardiograms a diffuse thickening of both ventricles was observed (Figure 3) with normal left ventricular ejection fraction and a dilated right ventricle with severely impaired function (TAPSE 4 mm). The filling pattern was restrictive with high filling pressures (E/E' 15). His New York Heart Association (NYHA) functional class declined to III-IV; he required several admissions between 2010 and 2012, and was treated with inotropic drugs and high-dose diuretics (Figure 4). Due to a lack of exact diagnosis, his physicians decided to perform a right catheterization (mPAP 34 mm Hg, PCWP 18 mmHg, CO 3.7 L/min, and PVR 4.4 Wood units) and repeat the biopsy ruling out rejection. The last blood test showed 9.2 g/dL Hb (29.6% Hto), stable renal function and high percentage of anti-human leucocyte antigen (HLA) antibodies (by luminex) (Figures 5 and 6).
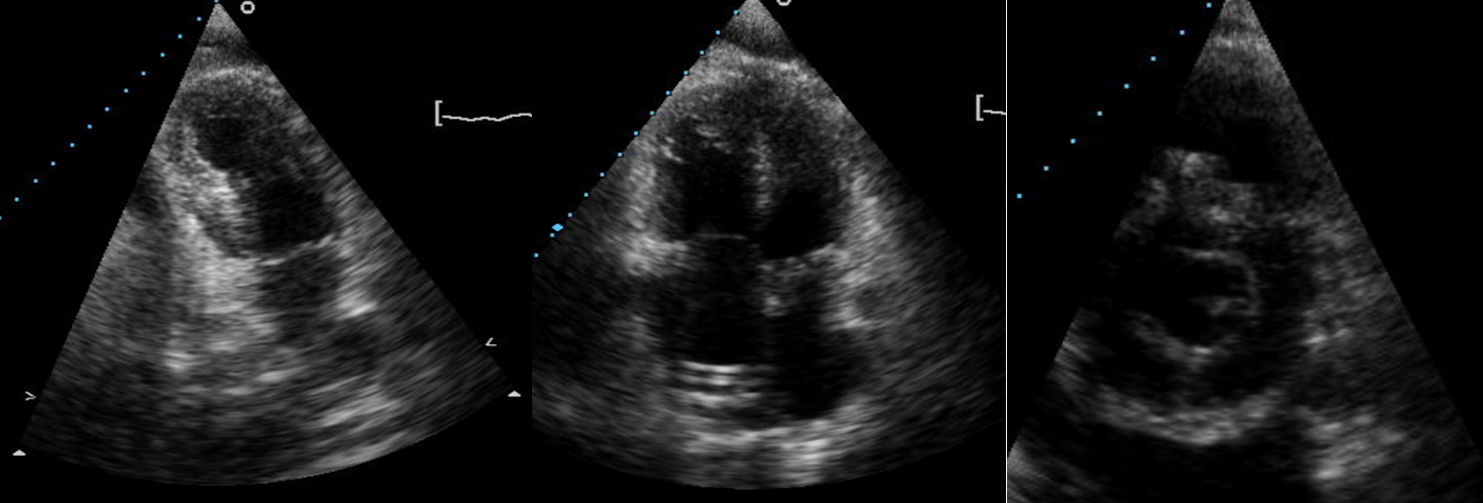
Figure 3
Diffuse thickening of both ventricles (left ventricle hypertrophy mainly) in two-chamber, four-chamber, and short-axis views.
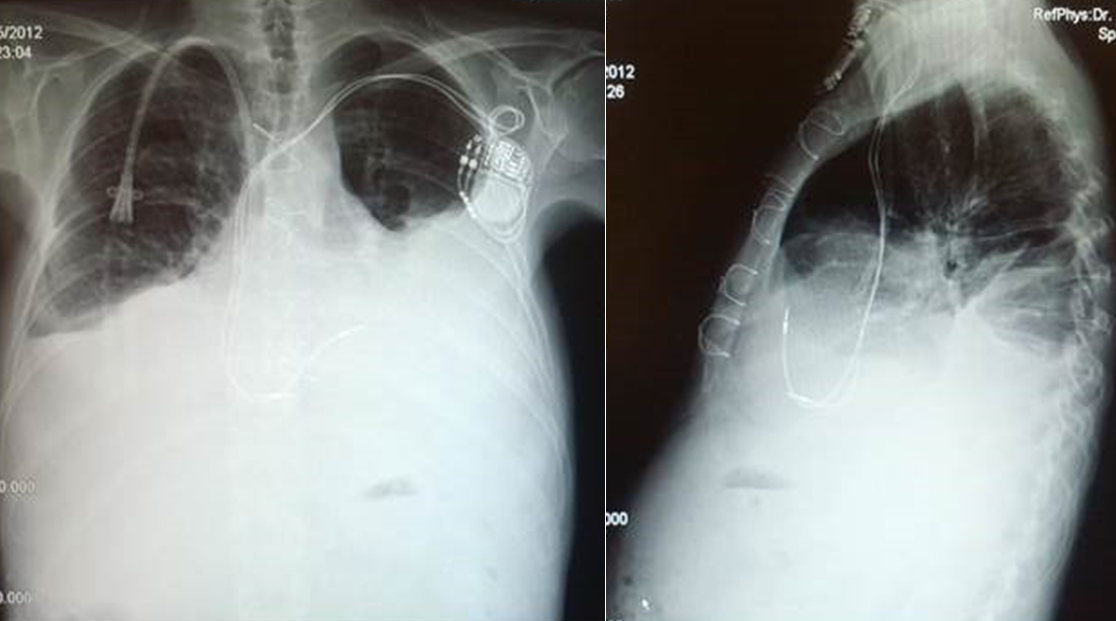
Figure 4
Postero-anterior and lateral chest X-ray images of the last admission. A bilateral massive pleural effusion can be seen.
Figure 5
Anti-HLA Type I Antibodies
Figure 6
Anti-HLA Type II Antibodies
Which of the following statements describes the best management in this situation?
Show Answer
The correct answer is: C. Treatment to reduce the concentration of antibodies and subsequent third heart transplant.
In this particular case, without any other contraindication for retransplantation, initial treatment to reduce the level of antibodies and subsequent inclusion in the heart transplant list was decided. After reduction to a secure level (four cycles of rituximab 375 mg/m2, 15 sessions of immunoadsorption, and three cycles of bortezomib 1.3 mg/m2), a third orthotropic heart transplant was performed requiring multiple transfusions due to severe coagulopathy. Finally the patient was discharged 30 days later with quadruple therapy (tacrolimus, mofetil mycophenolate, m-Tor inhibitor, and steroids). After 28 months, his clinical evolution is excellent.
Cardiac transplantation is still the only therapeutic treatment in end-stage heart failure patients. With the higher survival of these patients, the need for a second or third transplant is increasing progressively. The best way to assess a good retransplant result is to evaluate each patient individually, following the same protocol and the same requirements that were followed when considering the first transplant.1-4
The presence of anti-HLA class I and II antibodies, had been associated with a poor outcome after heart transplant. Multiple treatments are currently used for the management of these patients. Rituximab and immunoadsorption are used in those with very high levels.5-6
References
Lund LH, Edwards LB, Kucheryavaya AY, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-first official adult heart transplant report—2014; focus theme: retransplantation. J Heart Lung Transplant 2014;33:996-1008.
Topkara VK, Dang NC, John R, et al. A decade experience of cardiac retransplantation in adult recipients. J Heart Lung Transplant 2005;24:1745-50.
Atluri P, Hiesinger W, Gorman RC, et al. Cardiac retransplantation is an efficacious therapy for primary cardiac allograft failure. J Cardiothorac Surg 2008;3:26-31.
Copeland H, Coelho-Anderson R, Mineburg N, McCarthy M, Copeland JG. Elective cardiac retransplantation: a viable option that can be repeated. J Thorac Cardiovascular Surg 2011;141:822-7.
Ballew CC, Bergin JD. Management of patients with preformed reactive antibodies who are awaiting cardiac transplantation. Am J Crit Care 2005;14:46-51.
Singh N, Pirsch J, Samaniego M. Antibody-mediated rejection: treatment alternatives and outcomes. Transplant Rev. 2009;23:34-46.