Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
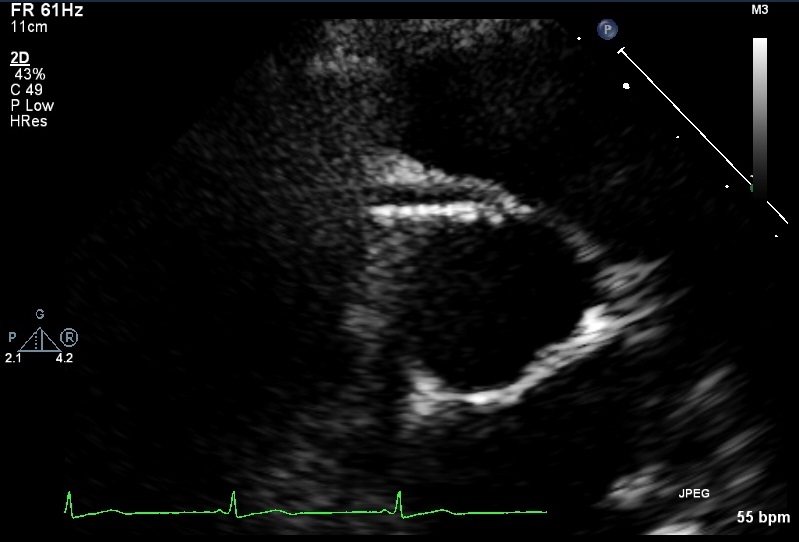
A 47-year-old female registered nurse with a family history of coronary artery disease presented with atypical chest pain and palpitations. The patient stated that she had been having chest pain that was sharp in nature, radiating to her left arm, not associated with exertion, and not associated with shortness of breath. Vitals and physical exam were grossly normal. She underwent a treadmill stress test during which she was able to exercise for 13.4 MET and achieved 98% of her maximal predicted heart rate. She had no symptoms, and the electrocardiogram tracings did not show any ischemic changes. The patient also had a Holter monitor as well as a Zio Patch, which revealed rare premature atrial contractions. Echocardiography was performed, which revealed normal biventricular ejection fraction, normal biatrial size, and no hemodynamically significant valvular heart disease. Abnormality visualized on the parasternal short axis view. The patient was then recommended to have a cardiac computed tomography angiography (CTA).
At this time, what would be the next course of action?
Show Answer
The correct answer is: E. Refer for surgical unroofing
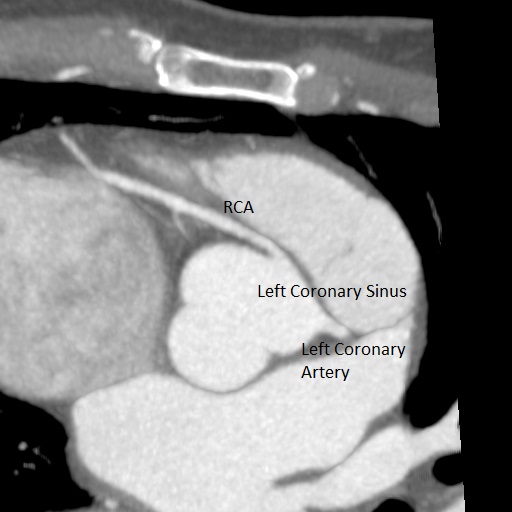
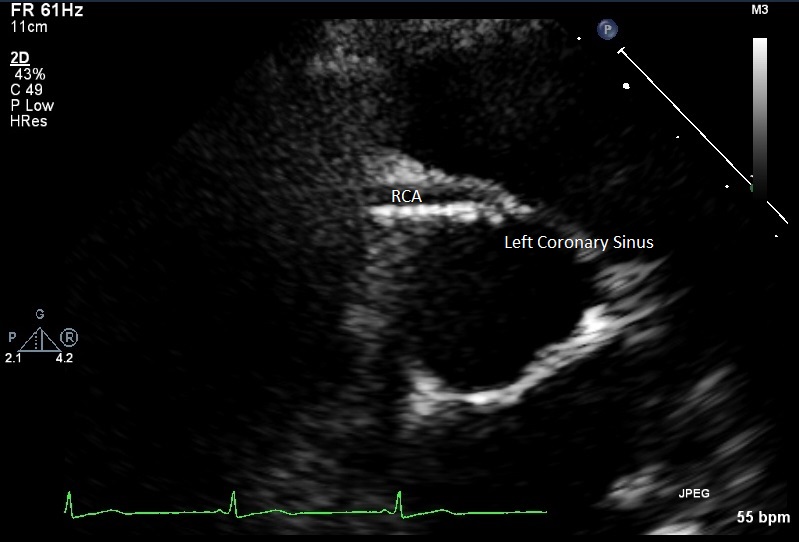
The echocardiogram and CTA reveal anomalous origin of the right coronary artery, arising from the left coronary sinus, traversing between the aorta and the pulmonary artery. In addition, the ostium of the artery appears to be slit-like (with narrowing of the ostial/proximal right coronary artery junction and a relative increase in size just distal to this). First reported by White and Edwards in 1948, it is a rare congenital anomaly with reported incidence of less than 1%. Cardiac CTA and cardiac magnetic resonance angiography are usually the best imaging modalities for visualizing coronary anomalies.
The pathophysiology of anomalous origin of the right coronary artery is complex and controversial, resulting in debates over the indications for surgery and the choice of surgical technique. Most patients are completely asymptomatic; however, some present with exertional angina or sudden cardiac death presumably relating to myocardial ischemia in the territory supplied by the artery. Characteristics that increase the risk of these outcomes include interarterial course, vasospasm, a slit-like ostium, and acute angle of take-off.1 Intravascular ultrasound has been utilized to identify certain high-risk characteristics as well, which include hypoplasia of intramural segments compared to extramural segments, lateral compression of intramural segment resulting in obstruction of artery.2 More recently, physiological modes of analysis such as fractional flow reserve (FFR) have been utilized to assess significance of anomalous origin of the right coronary artery. To fully assess the possible cause of dynamic obstruction, FFR with administration of dobutamine has also been studied in some smaller studies.3 Although in a small cohort, the studies have shown that there can be an improvement in the flow, as reflected by dobutamine stress FFR, after surgical repair of anomalous origin of the right coronary artery.
Currently, the recommendation of the American College of Cardiology and American Heart Association 2008 Guidelines for the Management of Adults With Congenital Heart Disease4 is to proceed with surgical intervention
in the symptomatic patient with evidence of myocardial ischemia, and
possibly in the asymptomatic patient with the presence of high-risk anatomic features (intramural course, interarterial course, slit-like ostium, or acute angulation of proximal coronary).
With regard to surgical revascularization, there are multiple techniques that can be utilized. If there is an intramural course of the anomalous artery, unroofing of the artery is the preferred method of surgical correction. If there is no intramural course, then reimplantation of the coronary or translocation of the pulmonary artery can be considered. More recently, there have been data that show that stenotic portions of anomalous right coronary artery may be treated with stent angioplasty.5
Our patient is currently awaiting surgical unroofing of the anomalous right coronary given her symptoms and presence of high-risk anatomic features.
References
Peñalver JM, Mosca RS, Weitz D, Phoon CK. Anomalous aortic origin of coronary arteries from the opposite sinus: a critical appraisal of risk. BMC Cardiovasc Disord 2012;12:83.
Angelini P, Velasco JA, Ott D, Khoshnevis GR. Anomalous coronary artery arising from the opposite sinus: descriptive features and pathophysiologic mechanisms, as documented by intravascular ultrasonography. J Invasive Cardiol 2003;15:507-14
Lee SE, Yu CW, Park K, et al. Physiological and clinical relevance of anomalous right coronary artery originating from left sinus of Valsalva in adults. Heart 2016;102:114-9.
Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Circulation 2008;118:e714-833.
Angelini P, Uribe C, Monge J, et al. Origin of the right coronary artery from the opposite sinus of Valsalva in adults: characterization by intravascular ultrasonography at baseline and after stent angioplasty. Catheter Cardiovasc Interv 2015;86):199-208.