A 17-year-old, previously healthy, Caucasian male reports one week of flu-like symptoms consisting of fevers, chills, and myalgias. On day 7 of his symptoms, he develops pleuritic chest pain and pressure and presents to the emergency department with the following electrocardiogram (Figure 1). His serial laboratory data reveals peak values of: troponin T 1.30ng/mL (normal 0.000-0.029ng/mL), CK 1000U/L (normal 30-220 U/L), CK-MB 87.6ng/mL (normal 30-220 U/L), CRP 3.3mg/dL (normal 0.0-1.0mg/dL), and WSR 9mm/hr (normal 0-10mm/hr). His creatinine and complete blood count (CBC) are normal. The patient undergoes transthoracic echocardiography which reveals normal biventricular function with a left ventricular ejection fraction (LVEF) of 60% and no evidence of pericardial effusion or valvular abnormalities. Left ventricular myocardial strain analysis is also normal. The same day, he undergoes a cardiac MRI (representative image in Figure 2), which suggests a lower LVEF than echo (52%), and reveals abnormal delayed enhancement imaging.
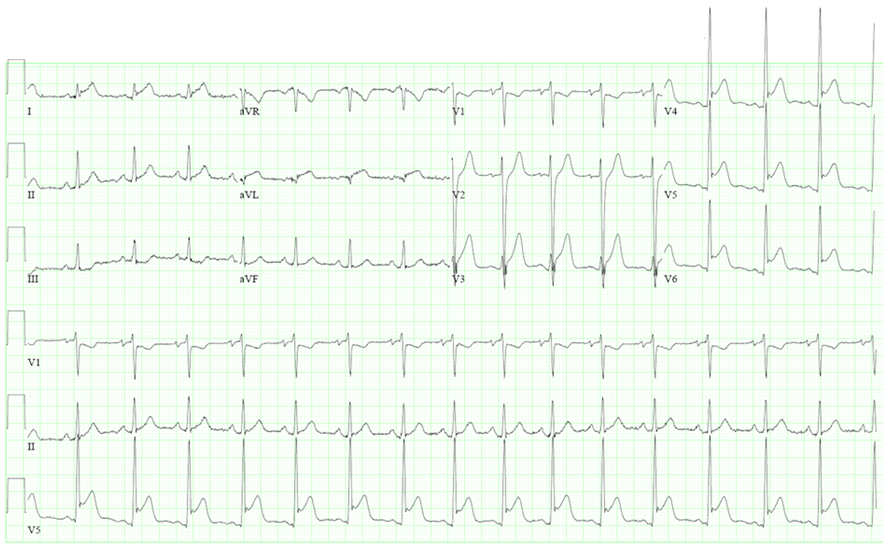
Figure 1: Presenting EKG
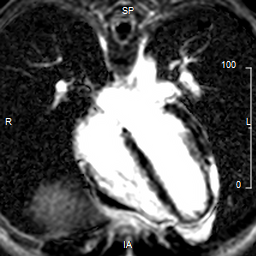
Figure 2: Cardiac MRI: four chamber delayed enhancement image
What is the most likely diagnosis?
Show Answer
The correct answer is: B. Perimyocarditis, focal
This patient presents with a pericardial syndrome. His presentation of acute, pleuritic chest pain 7 days following the onset of a flu-like illness with EKG changes of diffuse ST elevations and PR flattening is highly suggestive of post-infectious pericardial inflammation. Additionally, the elevated cardiac biomarkers and inflammatory markers suggest myocardial involvement and inflammation. The cardiac MRI image is a delayed-enhancement PSIR image that reveals focal, linear inferolateral and lateral wall enhancement with overlying pericardial enhancement, confirming the clinical diagnosis of focal perimyocarditis. Perimyocarditis and myopericarditis are often used interchangeably in the diagnosis of inflammatory pericardial conditions. However, to use these terms more precisely, one must recall that there is a continuum of pericardial disorders spanning pure pericarditis to pure myocarditis. Perimyocarditis suggests stronger myocardial involvement than pericardial involvement. Conversely, myopericarditis suggests stronger pericardial involvement than myocardial involvement. This young patient who was previously healthy has evidence of borderline LVEF of 52% for his age with moderate cardiac biomarker release, and MRI evidence of myocardial enhancement. All of the above suggest more myocardial involvement than pericardial involvement, which thus gives us the diagnosis of focal perimyocarditis.
The patient was treated with colchicine and NSAID therapy. He was seen for follow-up in 1 month, at which time his chest pain had improved. His ejection fraction has fully recovered to normal, and his inflammatory markers were within normal limits. He will continue to abstain from strenuous exercise to help reduce the recurrence of perimyocarditis for 6 months after initial diagnosis.
References
2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2015;36:2921-2964.
Buiatti A, Merlo M, Pinamonti B, De Biasio M, Bussani R, Sinagra G. Clinical presentation and long-term follow-up of perimyocarditis. J Cardiovasc Med (Hagerstown) 2013;14:235–241.
Childs H, Friedrich MG Cardiovascular magnetic resonance imaging in myocarditis. Prog Cardiovasc Dis. 2011;54:266–275.
Duraković Z, Misigoj Duraković M et al. Myopericarditis and sudden cardiac death due to physical exercise in male athletes. Coll Antropol.2008;32:399–401.
Cooper LT. Myocarditis. N Engl J Med 2009; 360:1526-1538
Imazio M, Brucato A, Barbieri A et al. Good prognosis for pericarditis with and without myocardial involvement: results from a multicenter, prospective cohort study. Circulation 2013 Jul 2;128(1):42-9
Imazio M, Spodick D, Brucato A, Trinchero R. Controversial issues in the management of pericardial diseases. Circulation 2010; 121: 916-928
Imazio M. Pericarditis with troponin elevation: is it true pericarditis and a reason for concern? J Cardiovasc Med (Hagerstown) 2014;15:73–77.
Imazio M, Brucato A, Spodick DH, Adler Y. Prognosis of myopericarditis as determined from previously published reports. J Cardiovasc Med (Hagerstown) 2014;15: 835–839.