Mr. Smith is a 58-year-old male patient with hypertension, dyslipidemia, stable ischemic heart disease, and type 2 diabetes mellitus. He presents to your clinic for routine follow-up of his stable ischemic heart disease. He has no new concerning cardiac symptoms and good exercise capacity.
His medications include aspirin 81 mg once daily, bisoprolol 5 mg once daily, perindopril 4 mg once daily, atorvastatin 40 mg once nightly, and metformin 1,000 mg twice daily.
His electrolytes and creatinine remain in the normal range. His low-density lipoprotein is at 60 mg/dL. His HbA1c is 8.3% (8.3% = 67 mmol/mol = 192 mg/dL).
Aside from further lifestyle advice, what additional pharmacotherapeutic strategy has been shown to improve both glycemic control and reduce cardiovascular events while lowering all-cause mortality?
Show Answer
The correct answer is: E. Both B and D
Both empagliflozin (a sodium-glucose cotransporter 2 inhibitor) and liraglutide (a glucagon-like peptide receptor agonist) have been shown to reduce cardiovascular events and all-cause mortality. The exact mechanisms of risk reduction are still being fully understood and elucidated but are likely multifaceted.
Empagliflozin promotes glycosuria, which has a net effect of lowering blood pressure and aiding weight loss through a physiologic natriuresis. A larger component of its effect on cardiovascular events and all-cause mortality may be attributed to reduction in heart failure-related deaths.
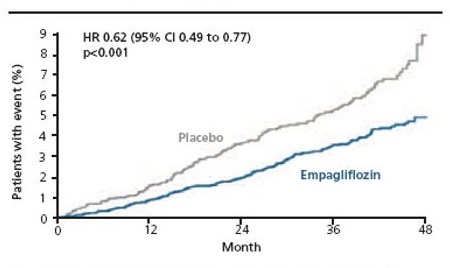
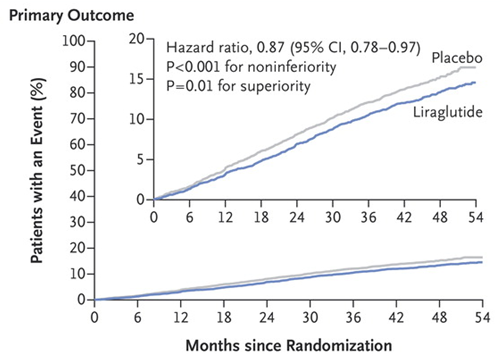
Liraglutide stimulates insulin release and delays gastric emptying, which also has a net effect of reducing blood pressure and promoting weight loss. In contrast to empagliflozin, there was no reduction noted in hospitalization for heart failure, but there were demonstrated reductions in major adverse cardiac event endpoints, likely driven by a reduction in non-fatal stroke. Interestingly, divergence of the survival curves for myocardial infarction and cardiovascular death were seen in just a few months after initiation of empagliflozin (Figure 1) versus at the 1-year mark for liraglutide (Figure 2).
Figure 1: The Cumulative Incidence of Death From Cardiovascular Causes in the Empagliflozin Group Versus Placebo Group in EMPA-REG OUTCOME
Hazard ratios (HR) are based on Cox regression analysis. Reproduced with permission from Zinman B et al.2
Figure 2
References
Valentine V. The Role of the Kidney and Sodium-Glucose Cotransporter-2 Inhibition in Diabetes Management. Clin Diabetes 2012;30:151-5.
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015;373:2117-28.
Marso SP, Bain SC, Consoli A, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016;375:1834-44.
Kosiborod M. Lower Rates of Hospitalization for Heart Failure and All-Cause Death in New Users of SGLT-2 Inhibitors: The CVD-REAL Study. Presented at 66th Annual ACC Scientific Session & Expo. March 17-19, 2017; Washington, DC.
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016;375;311-22.