A 14-year-old female with no known past medical history presents with twelve days of intermittent fever, rash, right lower quadrant pain, and neck pain. In the emergency department, she develops respiratory distress and hypotension; she is subsequently intubated and placed on inotropic support. Serum white blood cells and inflammatory markers are elevated. In the intensive care unit, she remains persistently febrile despite treatment with broad-spectrum antibiotics. Infectious workup is negative. Representative images from a transthoracic echocardiogram are shown (Figures 1 and 2). She undergoes treatment with intravenous pooled immunoglobulin and high-dose aspirin. She is weaned from inotropic support and, after three weeks, is discharged in stable condition on low-dose aspirin. Representative images from a follow-up cardiac magnetic resonance scan are shown (Figures 3 and 4).
Figure 1
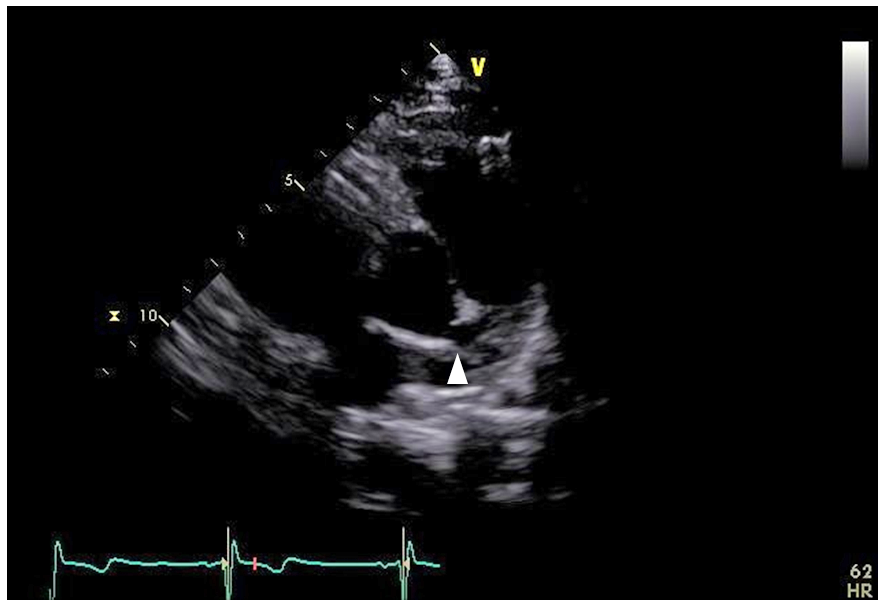
Figure 2
Figure 3
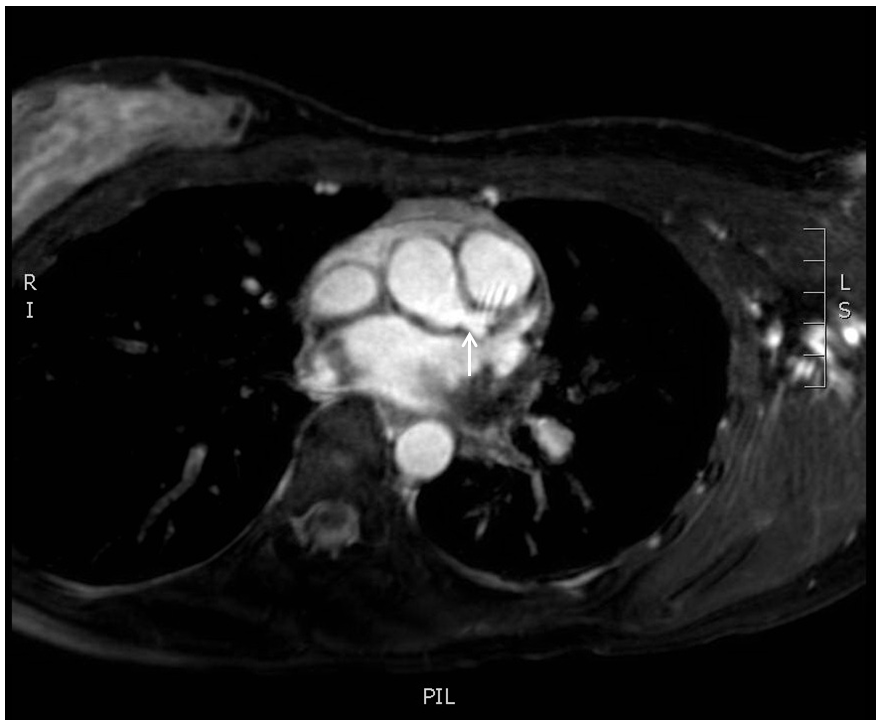
Figure 4
Which of the following statements describe the most likely diagnosis?
Show Answer
The correct answer is: B. Atypical/incomplete Kawasaki disease.
Kawasaki disease is a systemic vasculitis of childhood. Diagnostic criteria include the presence of fever for more than five days, along with at least four of the following five signs: bilateral conjunctival injection, oropharyngeal mucosal changes (e.g., strawberry tongue), peripheral extremity changes (e.g., arthritis, palmar erythema), polymorphous rash, and cervical lymphadenopathy. Treatment consists of intravenous immune globulin and aspirin.
Patients suspected of having Kawasaki disease yet lacking a sufficient number of the aforementioned diagnostic criteria are classified as having atypical or incomplete Kawasaki disease. Similar to patients with classic Kawasaki disease, patients with incomplete disease are at risk for cardiovascular complications including coronary artery aneurysm and dilatation, systolic dysfunction, and arrhythmia. Cardiac imaging, such as echocardiography and cardiac magnetic resonance, may support the diagnosis in cases of incomplete Kawasaki disease.
The present case illustrates one such scenario. In addition to fever, the patient exhibited only one of the five diagnostic criteria for Kawasaki disease (rash), yet she still progressed to hemodynamic collapse and responded to appropriate therapy. Echocardiography performed in the acute phase of the illness demonstrated coronary artery dilatation, with a proximal left main internal luminal diameter of 6 mm (Figure 1, white arrowhead), and a right coronary artery internal luminal diameter of 7 mm (Figure 2, white arrow). Indeed, these measurements meet Japanese Ministry of Health criteria for aneurysmal dilatation.
Follow-up cardiac magnetic resonance imaging, performed months later, demonstrated persistent coronary artery dilatation (Figures 3 and 4, white arrows). In accordance with guidelines, the patient was maintained on indefinite low-dose aspirin to prevent further coronary complications.
Viral myocarditis could certainly cause cardiovascular collapse in a young, otherwise healthy patient but would not cause the diffuse coronary enlargement seen on noninvasive imaging. Similarly, Still's disease and systemic-onset juvenile idiopathic arthritis could account for the patient's initial presentation of fever and rash; however, cardiovascular complications, including shock and coronary abnormalities, are rare.
Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004;110:2747-71.
Cimaz R, Sundel R. Atypical and incomplete Kawasaki disease. Best Pract Res Clin Rheumatol 2009;23:689-97.