A 56-year-old woman with history of hepatitis B presented to the emergency room with 12 hours of intermittent substernal chest pain preceded by a recent upper respiratory infection. She had an otherwise unremarkable medical history, and she was not taking any medications or supplements.
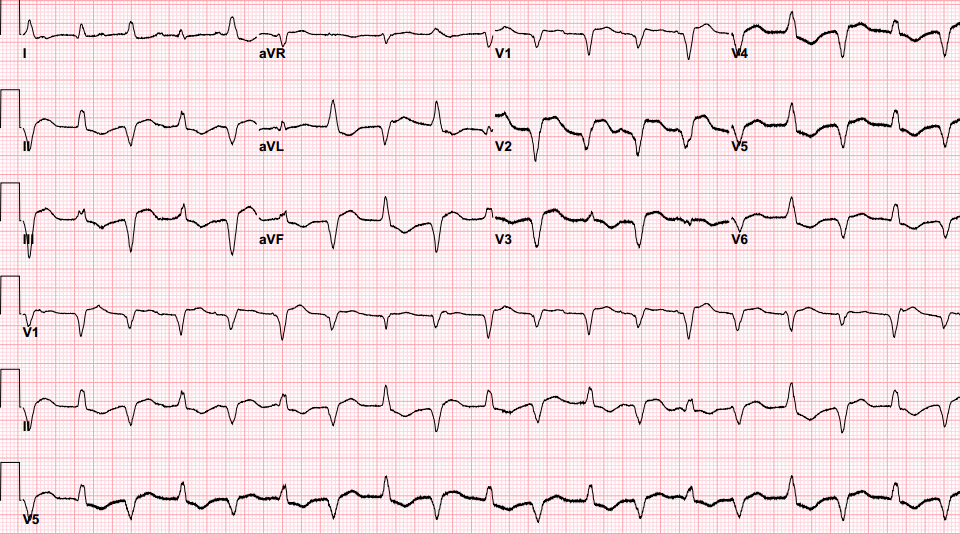
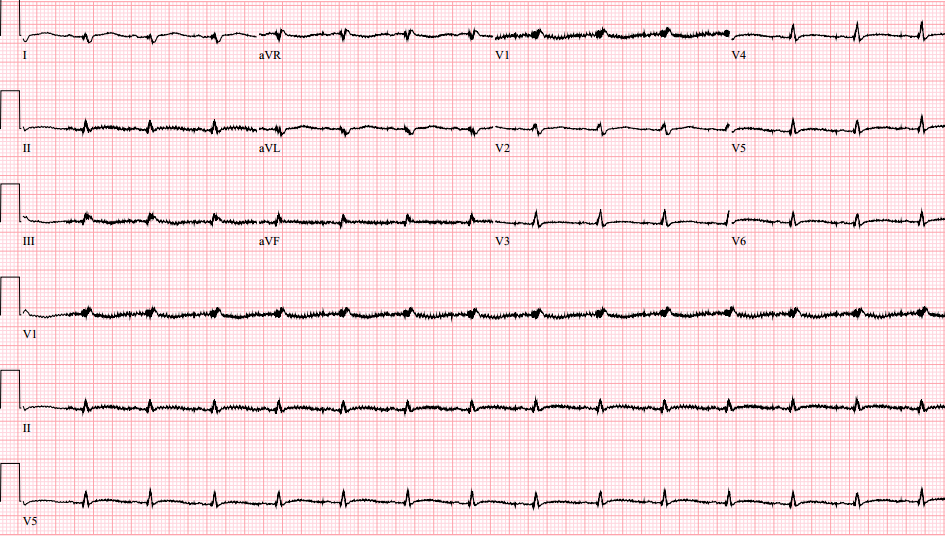
On admission, she was alert, awake and oriented but was noted to be tachycardic (heart rate 120 beats per minute [BPM]) and hypotensive (blood pressure [BP] 90/60 mm Hg) with cool, clammy extremities and 12 cm of jugular venous distension (JVD). Her physical exam was otherwise negative for murmurs, rubs, gallops, edema, or adventitious breath sounds. An electrocardiogram (ECG) in the emergency department showed bidirectional ventricular tachycardia (Figure 1). She was given 150 mg IV amiodarone bolus and started on a continuous infusion. The rhythm did not convert to sinus, but the ventricular rate slowed; her systolic BP remained ~90 mm Hg. Her bedside echocardiogram showed severely reduced global left ventricular systolic dysfunction (Videos 1 and 2). Initial troponin was 20 ng/ml and B-type natriuretic peptide (BNP) 644. Emergent left heart catheterization was performed and revealed non-obstructive coronary artery disease but confirmed a severely reduced LV systolic function with mid-inferior wall akinesis; LVEDP was 37 mm Hg. These findings were consistent with nonischemic cardiomyopathy with cardiogenic shock likely from acute myocarditis. Intra-aortic balloon pump was placed for hemodynamic support. A temporary transvenous pacemaker was also placed prophylactically for anticipated high-grade heart block. Six hours after presentation the patient developed complete heart block and transient asystole requiring the temporary back-up pacemaker.
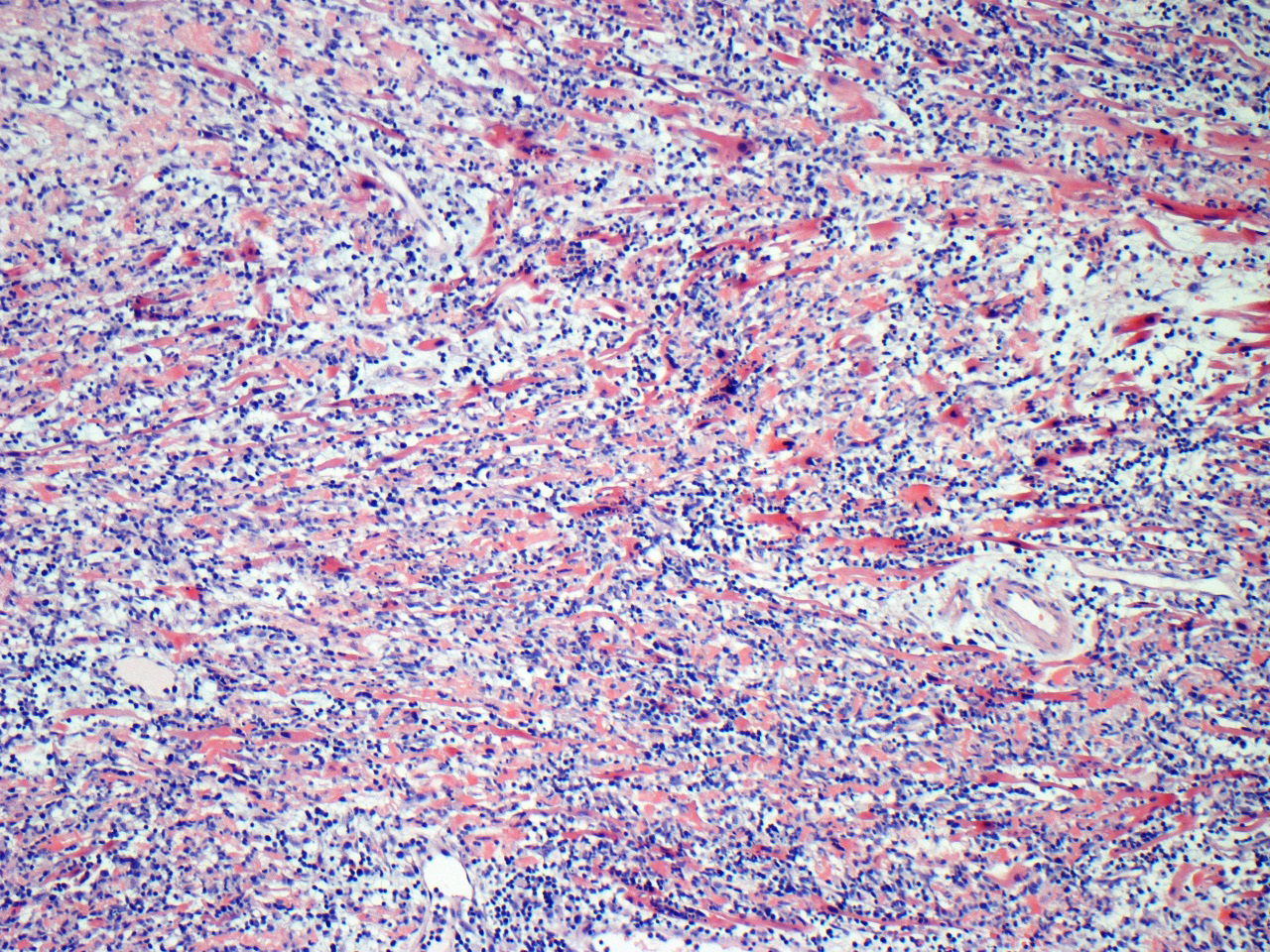
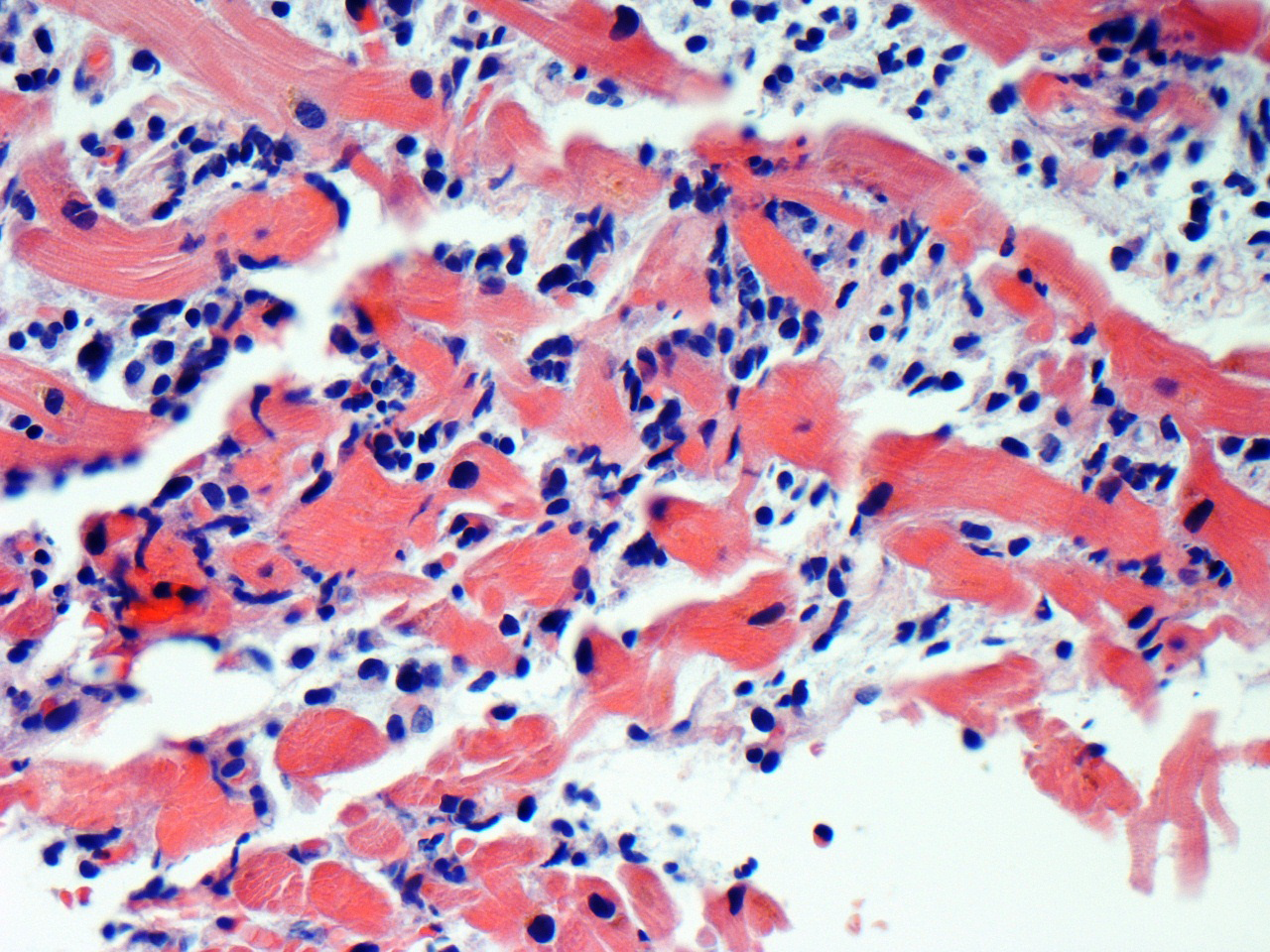
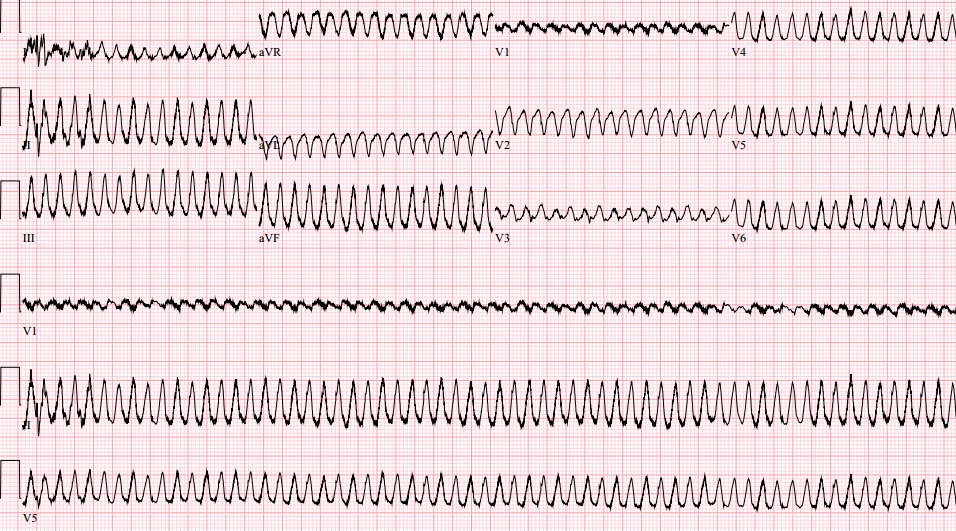
An endomyocardial biopsy revealed a severe lymphocytic myocarditis with significant myocyte damage (Figures 2 and 3). No etiological agents were identified. Despite increasing doses of inotropes, she remained hypotensive with oliguria. On hospital day 4, she underwent implantation of a Heart Mate II left ventricular assist device (LVAD; Thoratec Corporation, Pleasanton, CA) and required temporary right ventricular support with a CentriMag right ventricular assist device (RVAD; Thoratec Corporation, Pleasanton, CA). She had a prolonged postoperative course that included early sustained monomorphic ventricular tachycardia (Figure 4) which responded to amiodarone. Her RVAD was explanted on hospital day 17; she was discharged home with an LVAD on hospital day 39 in sinus rhythm (Figure 5).
Figure 1
Video 1
Video 2
Figure 2
Figure 3
Figure 4
Figure 5
Which of the following features of this case is consistent with fulminant myocarditis?
Show Answer
The correct answer is: A. Presentation with cardiogenic shock.
Answer Option A: Fulminant myocarditis presents abruptly with cardiogenic shock and often requires aggressive inotropic and mechanical circulatory support, and if the patient survives the acute phase, he or she generally has excellent long-term prognosis with histological and functional ventricular recovery.1,2 NYHA class, right ventricular dysfunction, pulmonary hypertension, and syncope are important clinical markers for increased mortality.3 and QRS duration greater than 120 ms is considered a poor prognostic sign.4 Immunosuppressive therapies are not of proven benefit in fulminant myocarditis. Mechanical circulatory support (ventricular assist devices) or extracorporeal membrane oxygenation should be promptly instituted as soon as it becomes clear that a patient has presented with fulminant myocarditis. This strategy provides the best chance of survival for the patient in the acute phase of fulminant myocarditis until they can be bridged to recovery or heart transplantation.
Answer Option B: A focal wall motion abnormality, if present on echocardiogram, goes against fulminant myocarditis. Patients with fulminant myocarditis characteristically have normal left ventricular end-diastolic dimension and increased thickness of the interventricular septum, possibly due to myocardial edema as opposed to those with nonfulminant myocarditis who have left ventricular dilation and normal wall thickness.5
Answer Option C: Lymphocytic infiltration on myocardial biopsy can be seen with both fulminant and nonfulminant myocarditis and, therefore, is not the correct answer. The Dallas criteria divides myocarditis into three histological categories: active myocarditis (lymphocytic infiltration and myocytolysis); borderline myocarditis (only lymphocytic infiltrate without myocytolysis); or negative (nomyocytolysis or lymphocytic infiltrate) but fails to clinically prognosticate these patients. Moreover, marked inter-observer variability severely limits its clinical utility in risk stratification of myocarditis. Viral serology and viral genome detection in myocardial tissue6 also has no specific prognostic value.
Answer Option D: Bidirectional ventricular tachycardia (BVT) is very rare in myocarditis. However, in the setting of the index presentation, it is important to recognize that bidirectional ventricular tachycardia (BVT) may be an early sign of the severe myocardial inflammation, and a temporary back-up pacemaker may be an important, although unconventional, consideration. As in this case, most reported cases for BVT in myocarditis (or other etiologies) are hemodynamically tolerated, pharmacologically treated, and rarely require emergent defibrillation. Although there is evidence that antitachycardia pacing may be an acceptable mode of management of this polymorphic ventricular tachycardia, there is no published report of the importance of a back-up pacemaker in the setting of a BVT in fulminant myocarditis with suspected unreliable escape rhythm as in our case.
BVT is a special type of polymorphic ventricular tachycardia characterized by an alternating beat-to-beat electrocardiographic QRS axis. It is classically associated with catecholaminergic polymorphic ventricular tachycardia (CPVT)7 and digoxin toxicity.8 Rarely has it been described in noncompaction cardiomyopathy.9 pulmonary embolism,10 myocardial ischemia,11 aconitine poisoning,12 familial hypokalemic periodic paralysis,13 fulminant myocarditis,14,15 and Andersen-Tawil syndrome (KCNJ2 gene mutations).16 Human and animal studies have shown that BVT is due to delayed after-depolarization induced triggered activity and alternating ectopic foci in His-Purkinje system ("reciprocating bigeminy").17 BVT has also been reported in pediatric studies of "occult myocarditis." Although there is only scant literature on BVT outside of CPVT and digoxin toxicity, it is thought to often portend a poor prognosis regardless of underlying etiology. Therefore, it becomes critically important to recognize its clinical implication in potentially reversible causes like myocarditis because it might be an early clue to a rather malignant course and distinguish it from more benign forms of acute and subacute myocarditis; this has major implications in management and outcome. Our case, heralded by BVT, is demonstrative of this fulminant course of myocarditis.
References
McCarthy RE 3rd, Boehmer JP, Hruban RH, et al. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med 2000;342:690-5.
Gupta S, Markham DW, Drazner MH, Mammen PP. Fulminant myocarditis. Nat Clin Pract Cardiovasc Med 2008;5:693-706.
Blauwet LA, Cooper LT. Myocarditis. Prog Cardiovasc Dis 2010;52:274-88.
Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M, Bohm M. Prognostic electrocardiographic parameters in patients with suspected myocarditis. Eur J Heart Fail 2011;13:398-405.
Felker GM, Boehmer JP, Hruban RH, et al. Echocardiographicfindings in fulminant and acute myocarditis. J Am Coll Cardiol 2000;36:227-32.
Mahfoud F, Gartner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011;32:897-903.
Francis J, Sankar V, Nair VK, Priori S. Catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm 2005;2:550–4.
Grimard C, De Labriolle A, Charbonnier B, Babuty D. Bidirectional ventricular tachycardia resulting from digoxin toxicity. J CardiovascElectrophysiol 2005;16:807-8.
Arias MA, Puchol A, Pachón M. Bidirectional ventricular tachycardia in left ventricular non-compaction cardiomyopathy. Europace 2011;13:962.
Tatli E, Aktoz M, Barutcu A, Altun A. Bidirectional tachycardia in a patient with pulmonary embolism. Cardiol J 2010;17:194-5.
Sonmez O, Gul EE, Duman C, Düzenli MA, Tokaç M, Cooper J. Type II bidirectional ventricular tachycardia in a patient with myocardial infarction. J Electrocardiol 2009;42:631-2.
Smith SW, Shah RR, Hunt JL, Herzog CA. Bidirectional ventricular tachycardia resulting from herbal aconite poisoning. Ann Emerg Med 2005;45:100-1.
Stubbs WA. Bidirectional ventricular tachycardia in familial hypokalaemic periodic paralysis. Proc R Soc Med 1976;69:223-4.
Chin A, Nair V, Healey JS. Bidirectional ventricular tachycardia secondary to subacute myocarditis. Can J Cardiol 2013;29:254.e13-4.
Berte B, Eyskens B, Meyfroidt G, Willems R. Bidirectional ventricular tachycardia in fulminant myocarditis. Europace 2008;10:767-8.
Kukla P, Biernacka EK, Baranchuk A, Jastrzebski M, Jagodzinska M. Electrocardiogram in Andersen-Tawil syndrome. New electrocardiographic criteria for diagnosis of type-1 Andersen-Tawil syndrome. Curr Cardiol Rev 2014;10:222-8.
Baher AA, Uy M, Xie F, Garfinkel A, Qu Z, Weiss JN. Bidirectional Ventricular Tachycardia: Ping Pong in the His-Purkinje System. Heart Rhythm 2011;8:599-605.
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012;59:779-92.