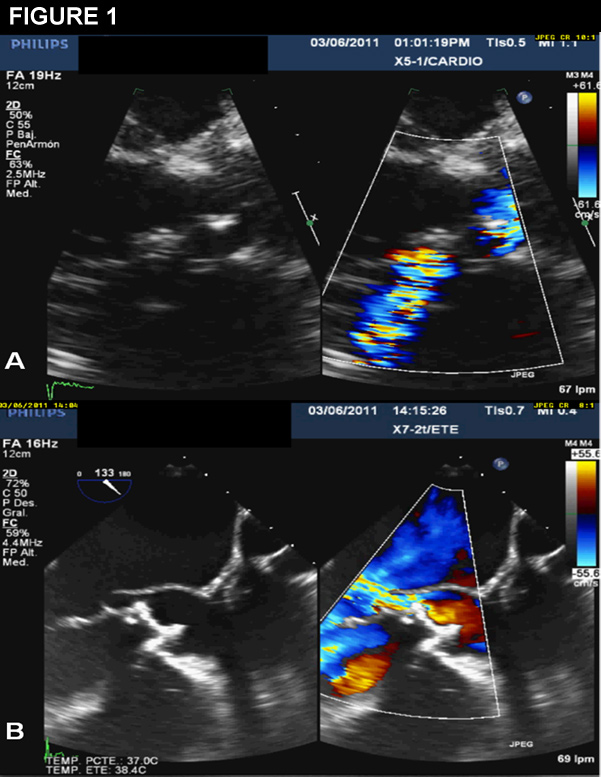
A 44-year-old male was referred to a cardiology outpatient clinic due to a six-month history of dyspnea on exertion and a cardiac murmur on physical examination. He underwent aortic valve replacement with a biological prosthetic valve and reconstruction of the mitro-aortic junction due to infective endocarditis by S. viridians in 2004, both events occurring in the same year. Transthoracic echocardiogram revealed a mild-dilated left ventricle with preserved function, a biological prosthetic valve with mild stenosis (effective area 1.3 mm
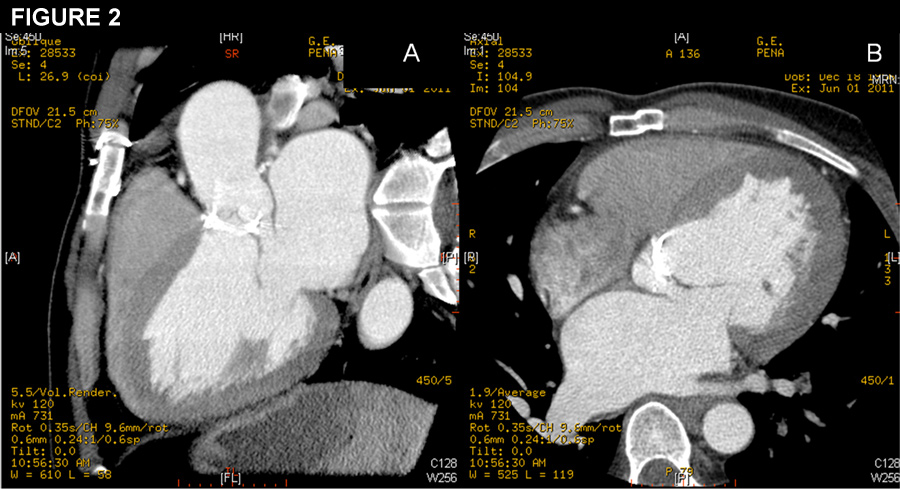
2) and an abnormal flow in left atrium (Figure 1, panel A). A transesophageal echocardiogram confirmed a patent communication between aortic root at level of non-coronary sinus and left atrium, close to the anterior mitral leaflet, with preserved prosthetic function (Figure 1, panel B). A 64-multislice CT demonstrated the defect and allowed the measurement of both long and short axis diameters (Figure 2, panels A and B).
The correct answer is: c. Percutaneous closure
This patient has a clinical and image findings corresponding with an aorto-atrial fistula, years after the surgery for endocarditis. Fistulas between aorta and cardiac cavities after infective endocarditis are rare. These aorto-cavitary communications create intra-cardiac shunts, which may result in clinical deterioration.1,2 Although surgery was the treatment by default years ago, such therapeutic option may carry serious complications and the mortality could be high.3 Percutaneous treatment represents an attractive alternative and the improvement of recent occlusion devices has placed this technique in the first line for the treatment of these defects.4 In this case, using right femoral approach we were able to cross the defect and we deployed two Amplatzer Vascular Plug III occluders. Monitorization with real-time 3D transesophageal echocardiography showed a marked decrease in the shunt magnitude and that both devices did not interfere with the mitral valve or aortic prosthetic valve function. On clinical follow-up, the patient is asymptomatic and echocardiographic controls revealed significantly decrease in the size of cardiac cavities.
References
- Anguera I, Miro JM, Vilacosta I et al. Aorto-cavitary fistulous tract formation in infective endocarditis: clinical and echocardiographic features of 76 cases and risk factors for mortality. Eur Heart J 2005:288-97.
- Anguera I, Miro JM, San Roman JA et al. Periannular complications in infective endocarditis involving prosthetic aortic valves. Am J Cardiol 2006:1261-8.
- Ananthasubramaniam K. Clinical and echocardiographic features of aorto-atrial fistulas. Cardiovasc Ultrasound 2005:1.
- Lu TL, Beregi JP, Rey C, Midulla M, Lions C. Percutaneous closure of an aorto-right ventricular fistula with an Amplatzer plug. J Vasc Interv Radiol 2011:100-1.