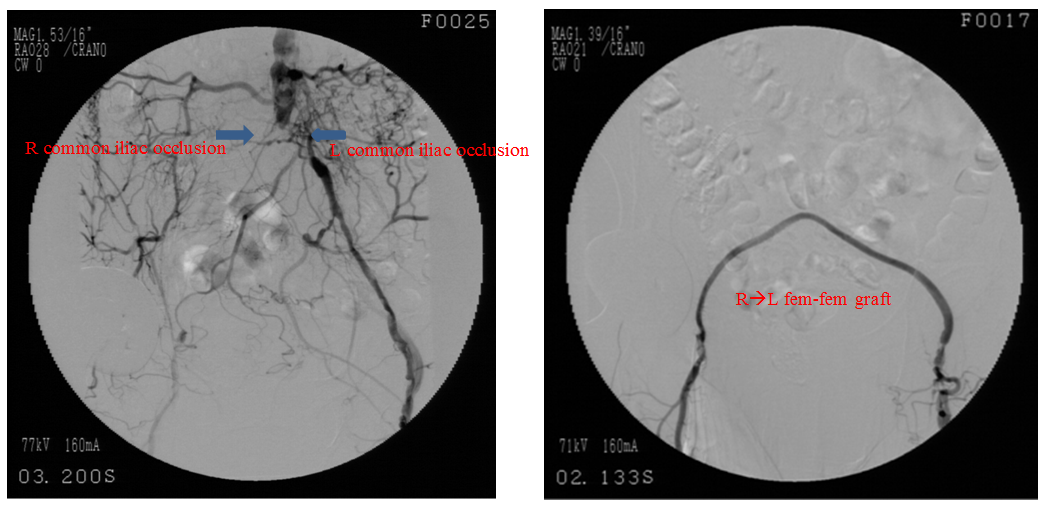
This case focuses on an 85-year-old female with a history of coronary artery disease (CAD) status post myocardial infarction and ventricular fibrillation with subsequent implantable cardioverter-defibrillator (ICD), hypertension, hyperlipidemia, and severe peripheral arterial disease status post multiple failed right iliac angioplasty/bare-metal stenting procedures and subsequent right-to-left femoral-femoral bypass. The patient presents with several months of worsening left foot pain and a non-healing left fourth toe ulcer. Ankle brachial index (ABI) of the left lower extremity is 0.00, suggesting a diagnosis of Rutherford class V critical limb ischemia. Angiography reveals bilateral iliac occlusion. The fem-fem bypass graft is patent but is non-functional due to a lack of right iliac inflow. She is evaluated by vascular surgery and is turned down for further surgical treatment other than possible amputation. She is referred to the interventional cardiology clinic for possible complex endovascular options.
Which of the following is a reasonable approach for endovascular intervention?
Show Answer
The correct answer is: D. All of the above.
This is a complex case of a patient with critical limb ischemia due to severe TransAtlantic Inter-Society Consensus (TASC) D inflow disease. Her right-to-left bypass graft was not being utilized appropriately due to her occluded right iliac stent. The complexity of this patient's disease and her designation as a poor surgical candidate place her outside of the realm of guideline-directed therapies.1
The best treatment option for TASC D lesions is controversial. The TASC II recommendations state that TASC A and B lesions should be treated endovascularly and TASC C and D lesions should be treated surgically.2 There is some accumulating data, however, suggesting that an initial endovascular approach regardless of TASC type (A-D) is appropriate.3-6 In the patient presented here, multiple different endovascular approaches could be reasonably attempted.
Answer Option A: Iliac artery in-stent restenosis (ISR) occurs with a frequency of approximately 10% at one year.7-8 There is no standardized treatment for iliac ISR; however, most lesions are treated with balloon angioplasty, cutting balloon, or re-stenting. One study found primary patency rates with balloon angioplasty of 88%, 62%, and 38% at one, three, and five years, respectively.9 Another study found 100% primary patency at two years after cutting balloon treatment for iliac ISR.10
Answer Option B: The use of covered stents in treating occlusive aorto-iliac disease is growing in popularity as the body of accumulating evidence has shown good outcomes. The randomized Covered Versus Balloon Expandable Stent Trial (COBEST) suggested that using covered stents rather than bare-metal balloon-expandable stents for TASC C and D lesions improved patency and clinical outcomes.11 One study showed excellent patency rates with covered stents in aortoiliac disease, but primary patency was worse if the covered stent was being used to treat ISR.12
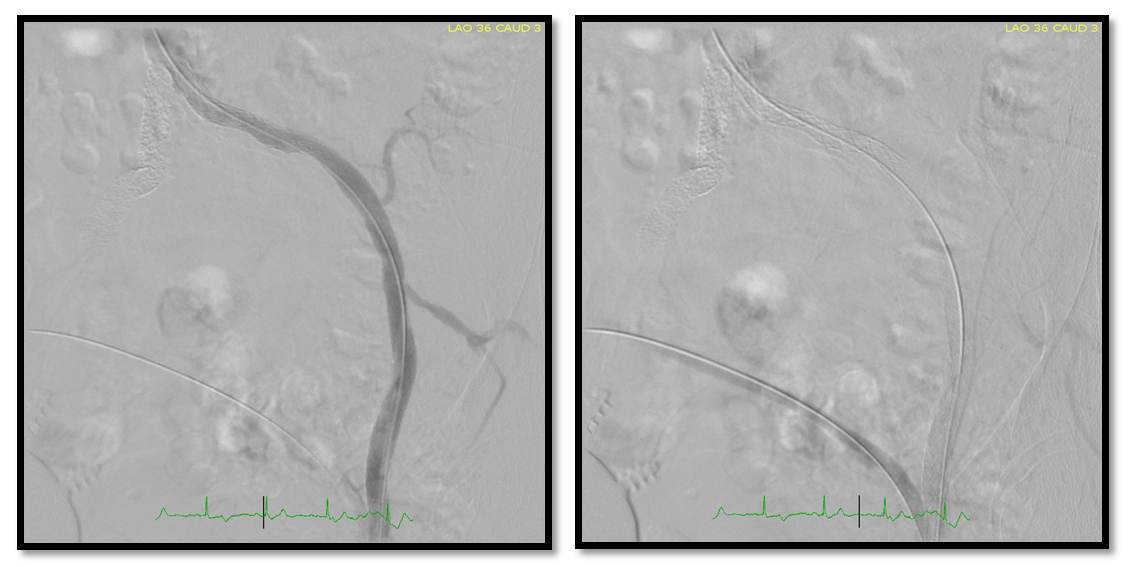
Answer Option C: The physicians chose to treat this patient by stenting the left iliac into the common femoral artery and reversing the flow of the bypass graft—initially right→left—to left→right. The physicians based this decision on multiple attempts at revascularization of the right iliac artery, and the data mentioned above suggesting stenting of de novo lesions has better patency than treatment of ISR. The patient tolerated the procedure well; at four-week follow-up, she was pain free and had significant improvement in her left foot ulcer. Her left ABI improved from 0.00 to 0.70.
Figures 3 & 4
References
Rooke TW, Hirsch AT, Misra S, et al. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;58:2020–45.
Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for management of peripheral artery disease (TASC II). J Vasc Surg 2007;45(suppl S):S5-S67.
Leville CD, Kashyap VS, Clair DG, et al. Endovascular management of iliac artery occlusions: extending treatment to TransAtlantic Inter-Society Consensus class C and D patients. J Vasc Surg 2006;43:32-9.
Sixt S, Alawied AK, Rastan A, et al. Acute and long-term outcome of endovascular therapy for aortoiliac occlusive lesions stratified according to the TASC classification: a single-center experience. J Endovasc Ther 2008;15:408-16.
Balzer JO, Gastinger V, Ritter R, et al. Percutaneous interventional reconstruction of the iliac arteries: primary and long-term success rate in selected TASC C and D lesions. Eur Radiol 2006;16:124-31.
Bosiers M, Deloose K, Callaert J, et al. BRAVISSIMO: 12-month results from a large scale prospective trial. J Cardiovasc Surg 2013;54:235-53.
Kudo T, Chandra FA, Ahn SS. Long-term outcomes and predictors of iliac angioplasty with selective stenting. J Vasc Surg 2005;42:466-475.
Koizumi A, Kumakura H, Kanai H, et al. Ten-year patency and factors causing restenosis after endovascular treatment of iliac artery lesions. Circ J 2009;73:860-866.
Kropman RH, Bemelman M, Vos JA, et al. Long-term results of percutaneous transluminal angioplasty for symptomatic iliac in-stent stenosis. Eur J Vasc Endovasc Surg 2006;32:634-8.
Tsetis D, Belli AM, Morgan R, et al. Preliminary experience with cutting balloon angioplasty for iliac artery in-stent restenosis. J Endovasc Ther 2008;15:193-202.
Mwipatayi BP, Thomas S, Wong J, et al. A comparison of covered vs bare expandable stents for the treatment of aortoiliac occlusive disease. J Vasc Surg 2011;54:1561-70.
Grimme FA, Spithoven JH, Zeebregts CJ, Scharn DM, Reijnen MM. Midterm outcome of balloon-expandable polytetrafluoroethylene-covered stents in the treatment of iliac artery chronic occlusive disease. J Endovasc Ther 2012;19:797-804.