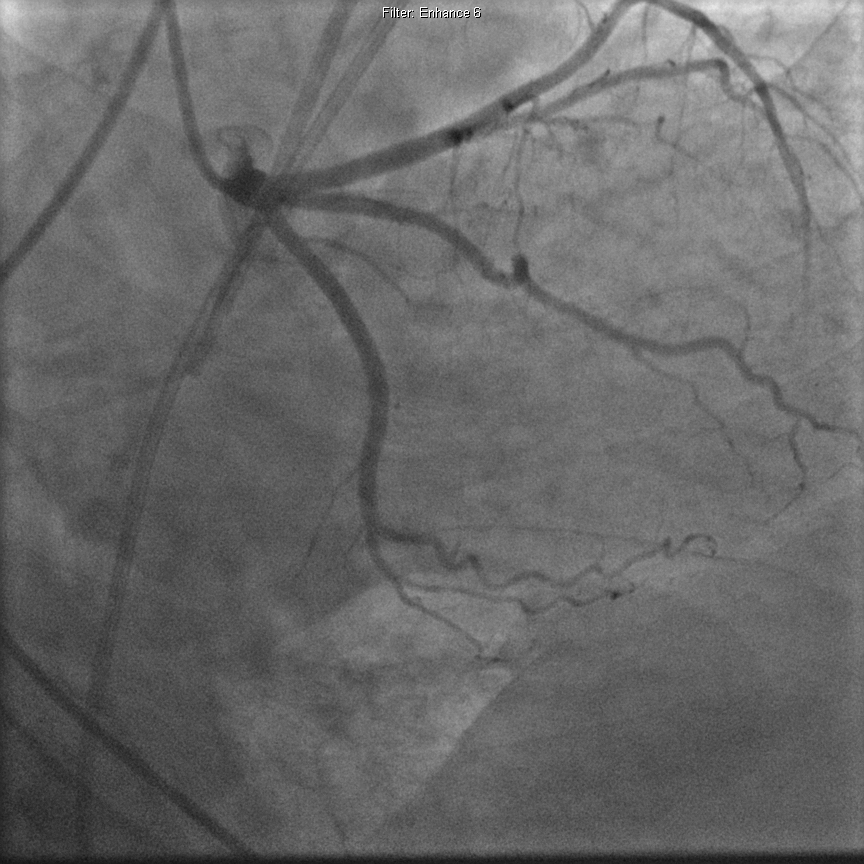
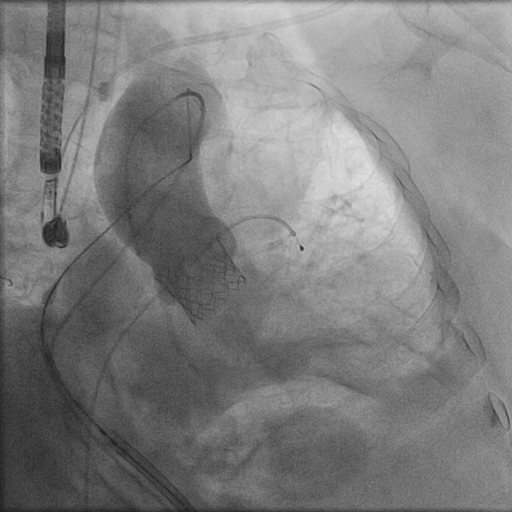
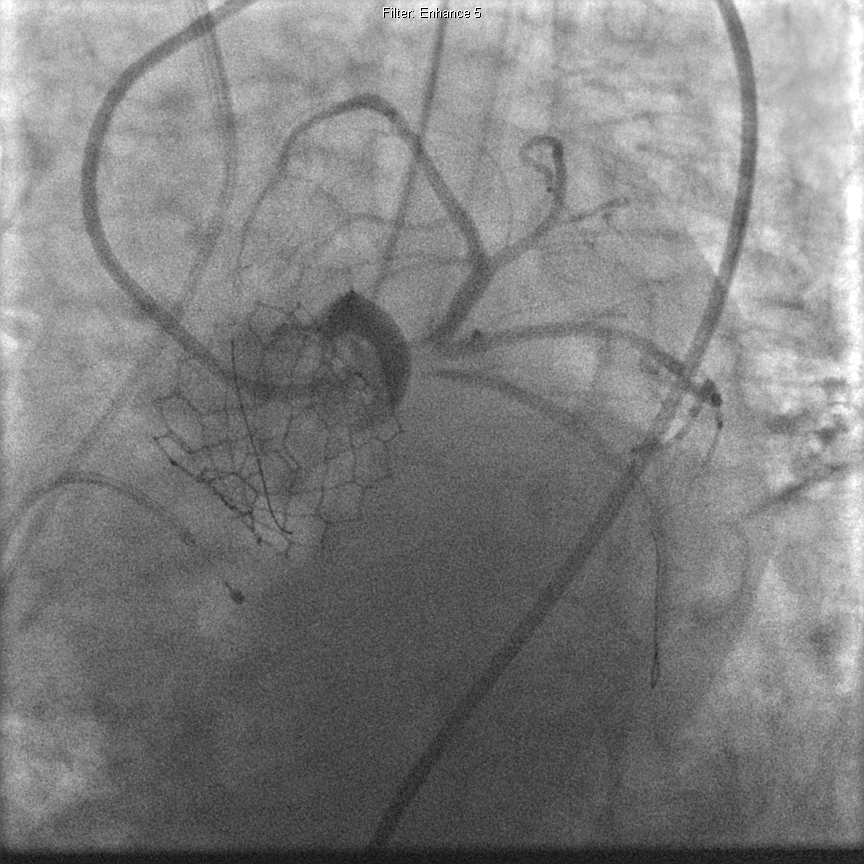
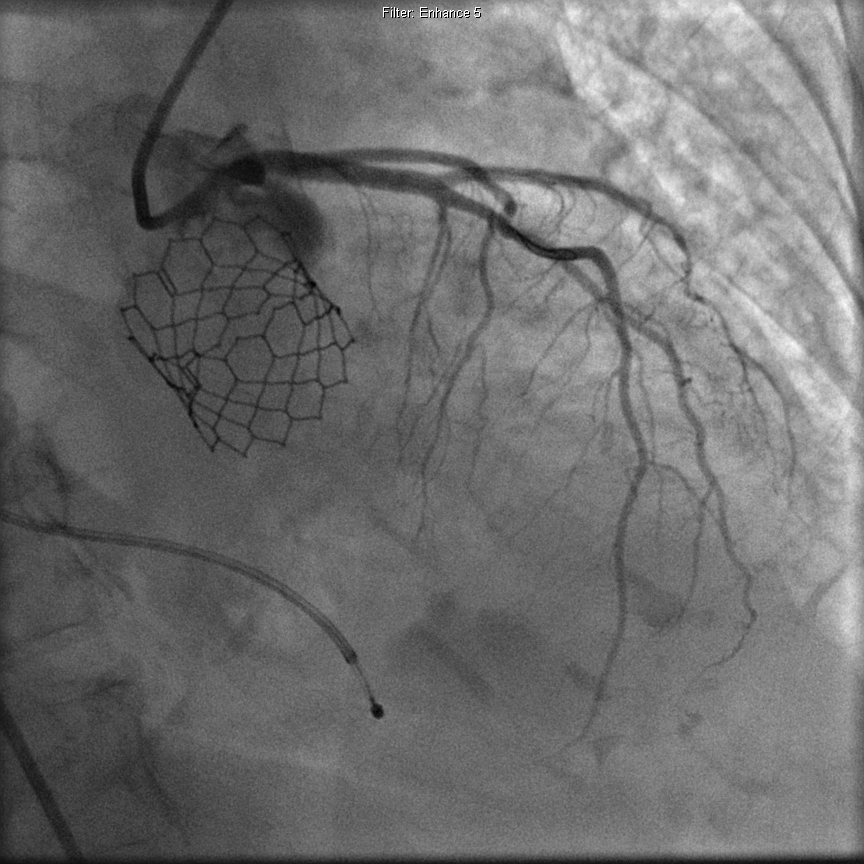
A 78-year-old female patient with prior medical history of hypertension, hyperlipidemia, and rheumatoid arthritis was admitted to the hospital with acute pulmonary edema and other signs and symptoms of congestive heart failure. A two-dimensional echocardiogram and left heart catheterization revealed low flow, low gradient severe aortic stenosis with a calculated valve area of 0.6 cm2 and preserved ejection fraction. Cardiac catheterization showed no evidence of coronary artery disease (CAD) (Figures 1-3). The patient underwent successful transcatheter aortic valve replacement (TAVR) via femoral approach using a balloon-expandable 26 mm Edwards SAPIEN 3 valve (Edwards Lifesciences, Inc., Irvine, CA) (Figure 4). The patient was in complete heart block post procedure and received a temporary pacer wire. A post-procedure echocardiogram showed a well-seated normally functioning prosthetic valve and normal ventricular function. Sixteen hours post-procedure, the patient developed epigastric discomfort accompanied by hypotension. An electrocardiogram was performed, which showed no evidence of acute ST-segment elevation myocardial infarction. A repeat bedside echocardiogram revealed an ejection fraction of 20% with akinesis in the apical, anterior, and anteroseptal wall segments (Video 1).
Figure 1: Coronary Angiography Prior to TAVR Showing no Underlying CAD
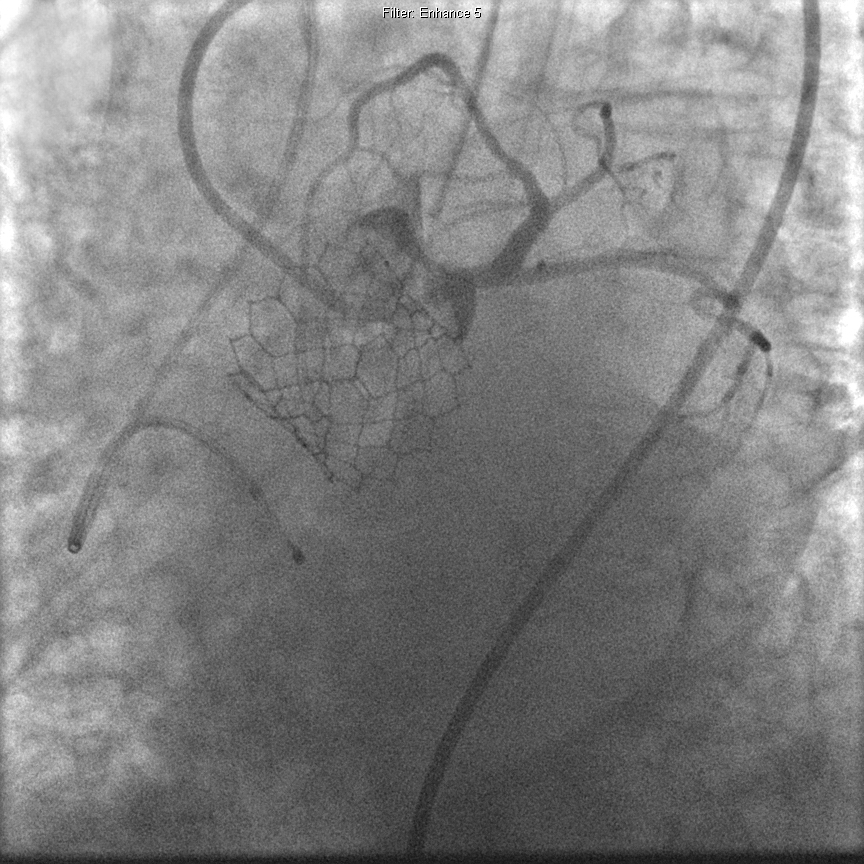
Figure 2: Coronary Angiography Prior to TAVR Showing no Underlying CAD
Figure 3: Coronary Angiography Prior to TAVR Showing no Underlying CAD
Figure 4: Aortogram Showing Successful Placement of a Balloon-Expandable Valve
Video 1: Presence of Wall Motion Abnormality in the Basal to Mid-Antero-Septal Segments on Echocardiogram in Parasternal Long-Axis View
What of the following should be considered in the differential diagnoses for development of acute hypotension following TAVR?
Show Answer
The correct answer is: E. All of the above
The patient's bioprosthetic aortic valve was functioning normally with no evidence of PVR on the repeat echocardiogram. The patient underwent emergent repeat cardiac catheterization, which revealed a new severe filling defect in the left main (LM) coronary artery extending into the left anterior descending (LAD) and left circumflex arteries (Figures 5-6). A 6F RunWay™ FL3.5 guide catheter (Boston Scientific Corporation, Marlborough, MA) was used to intubate the left coronary system. Following that, an ASASHI PROWATER 180 cm coronary guide wire (Abbott Laboratories, Abbott Park, IL) was used to cross the lesion across the LM into the LAD with relative ease. Balloon angioplasty was performed using 2 inflations, and a second generation 3.5 x 20 mm drug-eluting stent extending from the LM into the proximal LAD was placed successfully followed by post-dilation to re-establish coronary artery blood flow (Figures 7-8). Balloon angioplasty was attempted to address the ostial circumflex occlusion; however, it was unsuccessful due to an inability to cross the lesion through the LM stent. There were no procedure-related complications. The patient remained in cardiogenic shock for a brief amount of time receiving inotropes/pressors and was eventually discharged to a rehabilitation center after a prolonged in-hospital course. Follow-up echocardiogram 2 weeks later revealed improvement in ejection fraction (35-40%) with residual hypokinesis in the anterior, anteroseptal, apical, and anterolateral wall segment.
Figure 5: Coronary Angiography Post-TAVR Showing Acute Obstruction of the Proximal Left Coronary Artery System Including LM, LAD, and Left Circumflex Arteries
Figure 6: Coronary Angiography Post-TAVR Showing Acute Obstruction of the Proximal Left Coronary Artery System Including LM, LAD, and Left Circumflex Arteries
Figure 7: Coronary Angiogram With Re-Establishment of Coronary Blood Flow Following Successful PCI
Figure 8: Coronary Angiogram With Re-Establishment of Coronary Blood Flow Following Successful PCI
Acute shock may be triggered during or immediately following TAVR secondary to one or more of the following factors: use of sedatives and anesthesia, volume depletion including blood loss, rapid pacing, myocardial ischemia with ventricular dysfunction, and interruption in cardiac output during valve implantation. Other significant complications associated with TAVR in the immediate post-operative period include vascular complications, annular tears, bleeding, advanced conduction block requiring pacemaker implantation, significant residual PVR, stroke, embolic events, and death.1,2
Patients with acute aortic annular rupture may require emergent, open surgical root replacement or pericardial drainage and supportive care with close monitoring in the intensive care unit depending on severity.3
Moderate to severe PVR may be seen in up to a quarter of the cases following TAVR, especially in patients with heavily calcified annulus, undersized prosthesis, and suboptimal balloon dilation of aortic valve prior to deployment of prosthesis. Such patients are known to have a higher short- and long-term mortality compared with a patient with mild or no PVR.4
Currently, the most widely accepted mechanism causing acute coronary obstruction following TAVR is displacement of the native calcified cusp over the coronary ostium, resulting in acute ischemia and infarction. However, in our case we believe that the acute event was triggered from delayed embolization of calcific debris from the native valve. Ribeiro et al. found that female patients who received a balloon expandable valve were at higher risk for coronary obstruction following TAVR in a review of 24 reported cases.2 The left coronary artery was the most commonly involved artery, and involvement was more common with a low coronary artery ostial height (<10 mm), small sinuses, and extensive asymmetric valve calcification. The left coronary arterial ostial height was measured at 11.8 mm in our patient (Figure 9). Eleven of these patients did not have ST elevations on electrocardiogram and only 2 of 24 patients died while in hospital. Both these patients could not receive percutaneous coronary intervention (PCI) due to inability to cross with a wire requiring emergent coronary artery bypass grafting, eventually ending in cardiogenic shock and death. All patients with successful PCI were discharged from the hospital with no cases of repeat revascularization or stent thrombosis. They recommended measurement of the distance from aortic annulus to coronary ostium in cases prior to TAVR. Some practitioners recommend simultaneous aortography and pre-implant valvuloplasty to ensure patency of the coronary ostia in cases in which aortic root anatomy may suggest high risk of coronary flow impairment.5 Coronary obstruction is five times more frequent following valve-in-valve procedures compared with native aortic valve procedures (3.5 vs. 0.7%).6
Patients should be risk stratified prior to TAVR on the basis of measurement of distance from the aortic annulus to coronary ostium, measurement of sinus size, and extent and distribution of valvular calcification using a combination of imaging techniques such as cardiac catheterization and angiography, computed tomography, and three-dimensional transesophageal echocardiography. PCI remains the first line of treatment for coronary obstruction when feasible, and additional hemodynamic support and conversion open heart surgery may be needed in some cases. In our experience in high-risk cases, provisional placement of an uninflated balloon into the left coronary system may assist in timely reversal and management of acute left coronary artery obstruction that occurs immediately in the setting of valve implantation.
Figure 9: Computed Tomography Scan of the Aortic Root Demonstrating Measurement of the Left Coronary Artery Ostial Height
References
Généreux P, Head SJ, Van Mieghem NM, et al. Clinical outcomes after transcatheter aortic valve replacement using valve academic research consortium definitions: a weighted meta-analysis of 3,519 patients from 16 studies. J Am Coll Cardiol 2012;59:2317-26.
Ribeiro HB, Nombela-Franco L, Urena M, et al. Coronary obstruction following transcatheter aortic valve implantation: a systematic review. JACC Cardiovasc Interv 2013;6:452-61.
Eker A, Sozzi FB, Civaia F, Bourlon F. Aortic annulus rupture during transcatheter aortic valve implantation: safe aortic root replacement. Eur J Cardiothorac Surg 2012;41:1205.
Pibarot P, Hahn RT, Weissman NJ, Monaghan MJ. Assessment of paravalvular regurgitation following TAVR: a proposal of unifying grading scheme. JACC Cardiovasc Imaging 2015;8:340-60.
Barbanti M. Avoiding coronary occlusion and root rupture following TAVI- The role of pre-procedural imaging and prosthesis selection. Interventional Cardiology Review 2015;10:94-7.
Webb JG, Dvir D. Transcatheter aortic valve replacement for bioprosthetic aortic valve failure: the valve-in-valve procedure. Circulation 2013;127:2542-50.