Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
A two-day-old, full-term infant was transferred to a level 3 neonatal intensive care unit (NICU). She did well until 36 hours of life, at which time she developed marked tachypnea with grunting and retractions. Serum glucose was 95 mg/dL (normal). Lower extremity pulse oximetry was 88%. She was placed on oxygen by nasal cannula with no significant change. Blood and urine cultures were obtained, antibiotics administered, and transfer arranged. Prostaglandin E-1 was initiated, but the infant continued to decline with worsening SpO2, requiring intubation.
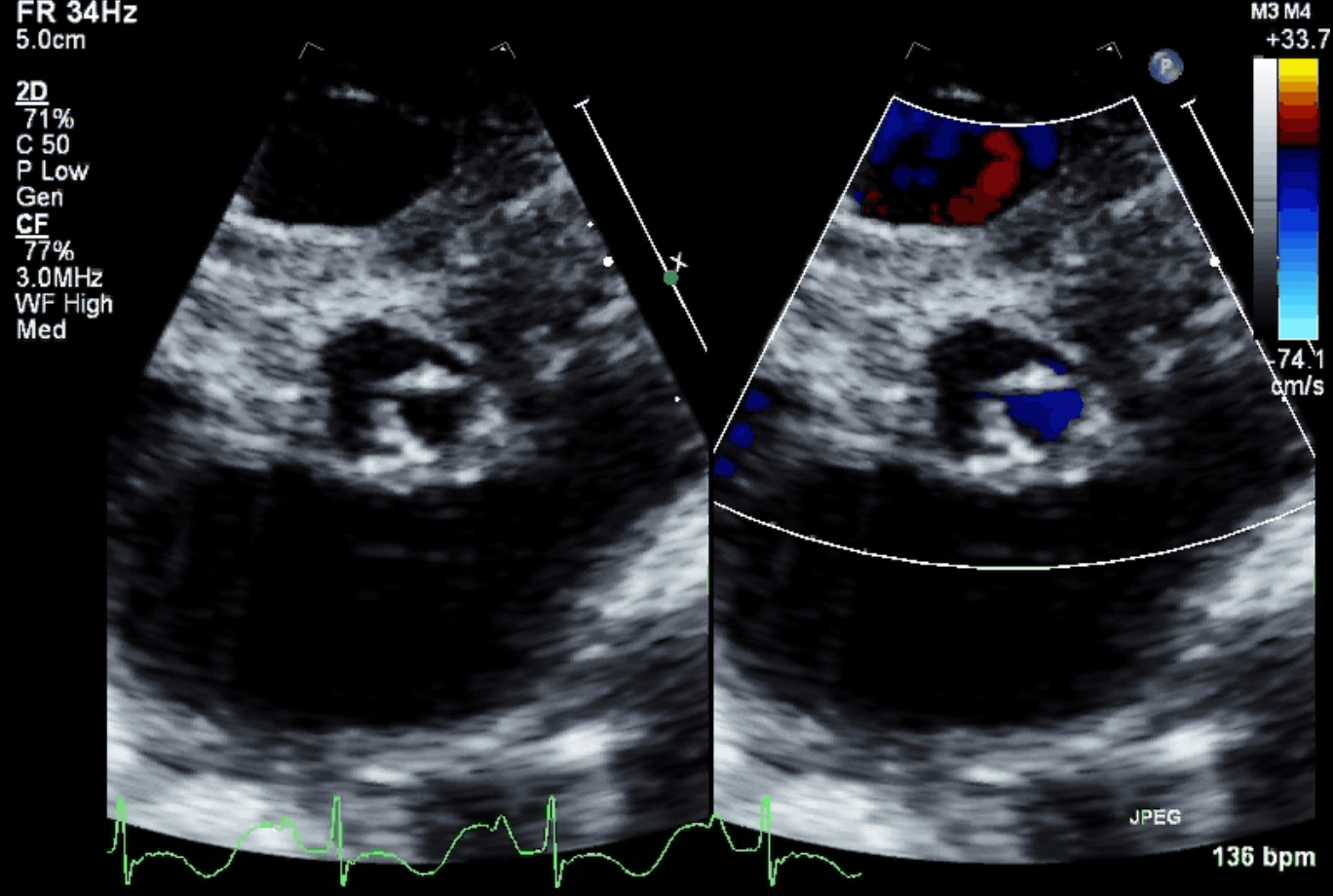
Figure 1
Patient's aortic valve (parasternal short axis)
Upon arrival, Heart rate was 166 BPM. All four extremity systolic blood pressures were in the 60s (mm Hg). Pre- and post-ductal SpO2 on 50% Fi02 were 88% and 84%, respectively. There was good air entry and clear lung fields, with a right ventricular (RV) heave and normal S1 but a loud, split S2. There was a harsh II-III/VI continuous murmur at the left upper sternal border that radiated throughout the precordium. There was no brachiofemoral delay. An arterial blood gas (ABG) demonstrated pH 7.31, pCO2 47, and pO2 42; with lactate 4.5 mmol/L. An echocardiogram was performed (Figure 1).
Which of the following echocardiographic parameters is best associated with a successful biventricular repair in this case?
Show Answer
The correct answer is: D. Mitral valve area (indexed).
The patient has critical aortic stenosis (AS) due to a unicommissural aortic valve. The incidence of AS ranges from 0.04 to 0.38 per 1000 live births, with an approximately 4:1 male predominance. Many cases are secondary to a dysplastic, bicommissural aortic valve. Thickening of the valve cusps is a common finding; however, as opposed to adult cases, calcification is rare in children.1,2
In critical AS, infants present with signs of inadequate cardiac output, congestive heart failure, and LV dysfunction with ductal dependence for systemic circulation. Patients with critical AS may not have a high gradient across the aortic valve due to left ventricular dysfunction, leading to a low stroke volume and, therefore, a relatively "low" transaortic gradient despite severe obstruction.3,4
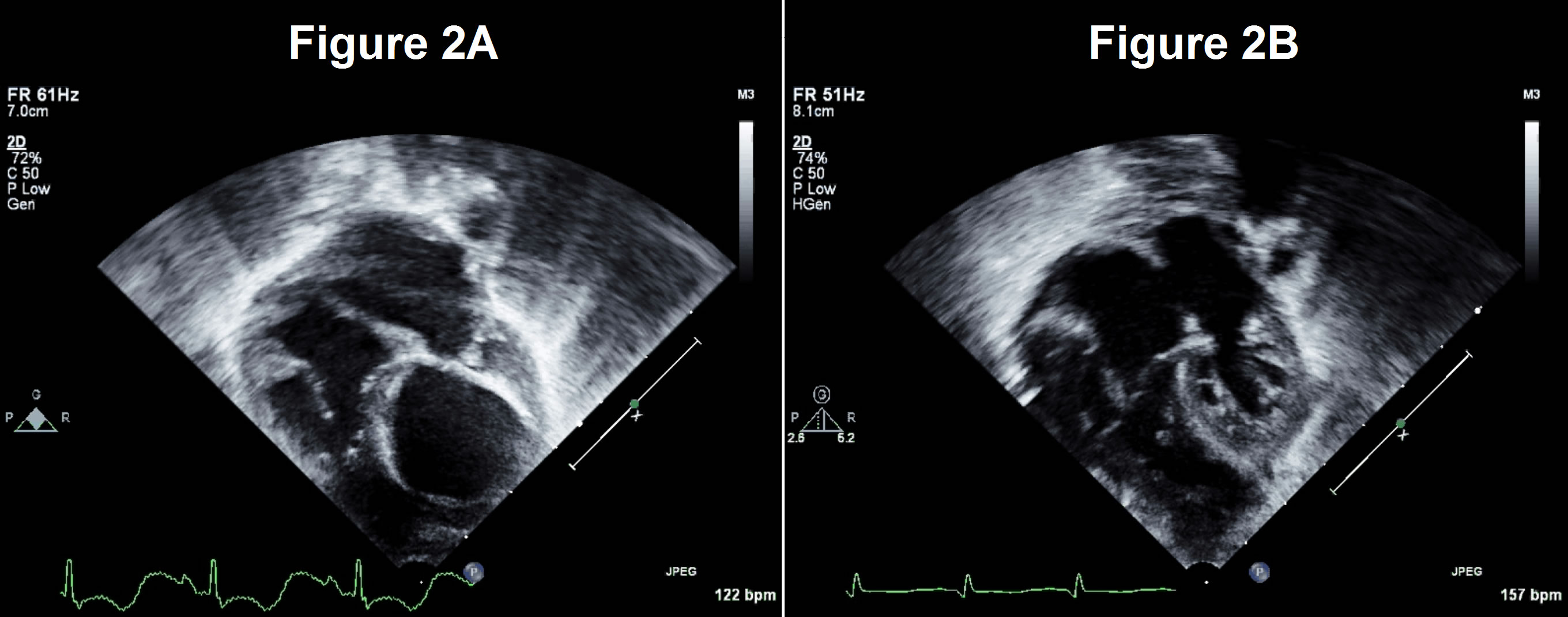
Figures 2A/2B
Patient's heart in apical four-chamber views, before (A) and after (B) stage 1
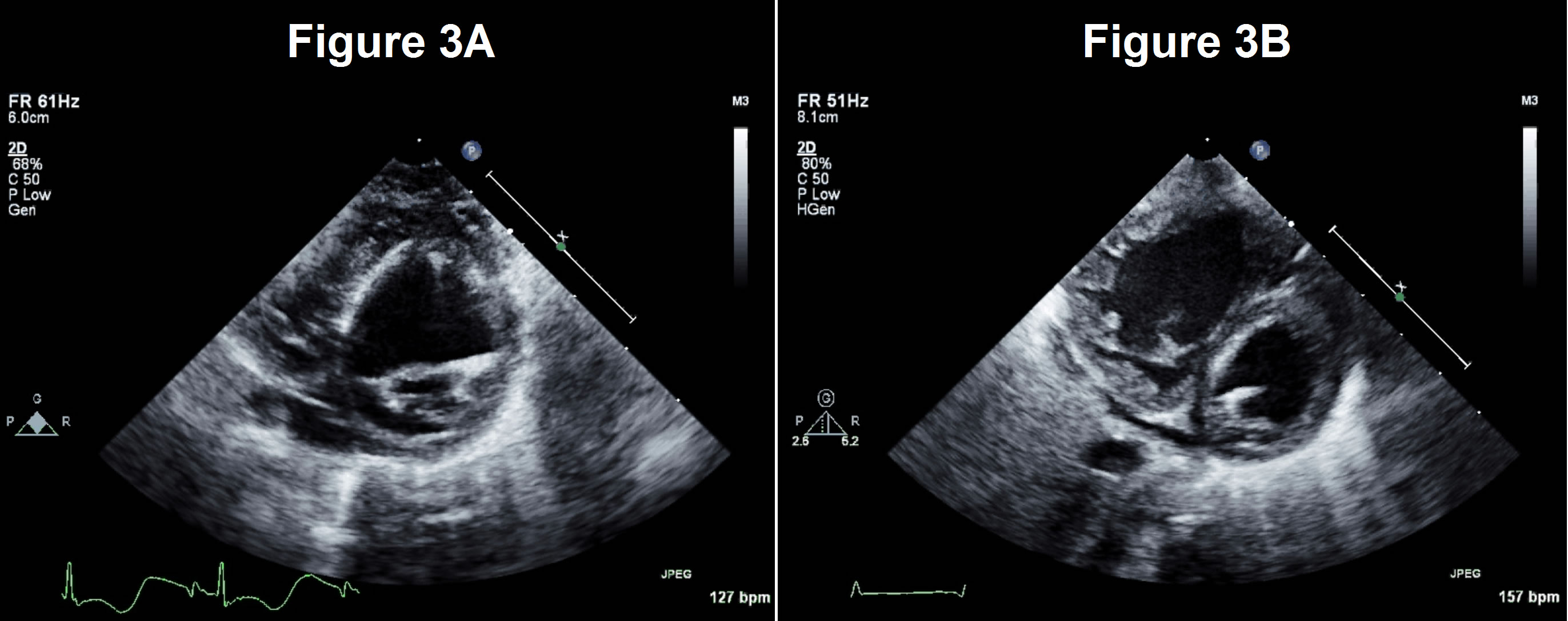
Figures 3A/3B
Patient's heart in parasternal short-axis views, before (A) and after (B) stage 1
In a sentinel paper, Rhodes et al. investigated parameters associated with successful biventricular repair in patients with critical AS. Eleven parameters were analyzed, but there was significant overlap among groups that precluded establishing a lower-limit threshold using any single measure. However, survival after a two-ventricle repair had a 90% accuracy using mitral valve area, LV long-axis to total heart length ratio, and aortic root size as criteria.5 Thus, the correct answer is D.
Some patients with critical AS may suffer higher complication rates if an initial two-ventricle repair strategy is undertaken. Early re-intervention (within 30 days) after the index procedure was associated with high risk of mortality.6 LV dysfunction, subvalvar obstruction, fewer aortic valve cusps, and a larger tricuspid valve annulus were associated with high risk of early first re-intervention.6,7,9 Endocardial fibroelastosis (EFE), a thickening of the endocardium from deposition of collagen and elastic fibers, is another factor strongly associated with increased morbidity and mortality.10-13 Overall, these findings suggest that a "trial" attempt at biventricular repair may be high-risk in patients with these findings, with greater likelihood of survival by pursuing a single-ventricle repair strategy.
This patient had a hypoplastic mitral valve (Z-score -2.4), a unicommisural aortic valve and significant EFE (Figures 2a and 3a). He underwent a stage 1 single-ventricle palliation. Subsequent studies show a significant decrease in LV size and more pronounced EFE after decompression, suggesting that the left heart was incapable of supporting systemic circulation (Figures 2b and 3b). The patient is currently doing well.
Allen HD, Driscoll DJ, Shaddy RE Moss & Adams' Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adult. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
Lofland GK, McCrindle BW, Williams WG, et al. Critical aortic stenosis in the neonate: A multi-institutional study of management, outcomes, and risk factors. J Thorac Cardiovasc Surg 2001;121:10-27.
Hammel JM, Duncan KF, Danford DA, Kutty S. Two-stage biventricular rehabilitation for critical aortic stenosis with severe left ventricular dysfunction. Eur J Cardiothorac Surg 2013;43:143-8.
Rhodes LA, Colan SD, Perry SB, Jonas RA, Sanders SP. Predictors of survival in neonates with critical aortic stenosis. Circulation 1991;84:2325-35.
Hickey EJ, Caldarone CA, Blackstone EH, et al. Biventricular strategies for neonatal critical aortic stenosis: High mortality associated with early reintervention. J Thorac Cardiovasc Surg 2012;144:409-17.e1.
Hickey EJ, Caldarone CA, Blackstone EH, , et al. Critical left ventricular outflow tract obstruction: The disproportionate impact of biventricular repair in borderline cases. J Thorac Cardiovasc Surg 2007;134:1429-36; discussion 1436–7.
Reich O, Tax P, Marek J, et al. Long term results of percutaneous balloon valvoplasty of congenital aortic stenosis: independent predictors of outcome. Heart Br Card Soc 2004;90:70-6.
Bhabra MS, Dhillon R, Bhudia S, et al. Surgical aortic valvotomy in infancy: impact of leaflet morphology on long-term outcomes. Ann Thorac Surg 2003;76:1412-6.
Lurie PR. Changing concepts of endocardial fibroelastosis. Cardiol Young 2010;20:115-23.
Agnoletti G, Raisky O, Boudjemline Y, et al. Neonatal surgical aortic commissurotomy: predictors of outcome and long-term results. Ann Thorac Surg 2006;82:1585-92.
Colan SD, McElhinney DB, Crawford EC, Keane JF, Lock JE. Validation and re-evaluation of a discriminant model predicting anatomic suitability for biventricular repair in neonates with aortic stenosis. J Am Coll Cardiol 2006;47:1858-65.
Brown JW, Ruzmetov M, Vijay P, Rodefeld MD, Turrentine MW. Closed transventricular aortic valvotomy for critical aortic stenosis in neonates: outcomes, risk factors, and reoperations. Ann Thorac Surg 2006;81:236-42.