68-year-old male without a significant cardiac history was diagnosed with atrial fibrillation (AF) 12 years ago (at age 56). Initially the episodes were 3-4 times/year but over the next few years the paroxysms increased to weekly. No precipitating factors identified. Initially treated with beta blockers with moderate success and approximately 5 years ago propafenone was added which suppressed most of the episodes. However, six months ago the paroxysms of AF returned and propafenone was changed to amiodarone. Unfortunately, the AF continued. The episodes last from 1-4 hours. He was referred to the Atrial Fibrillation Center for management.
SHx: retired physician, exercises 3X week for 30 min on an elliptical, no smoking, alcohol averages 4 drinks/week
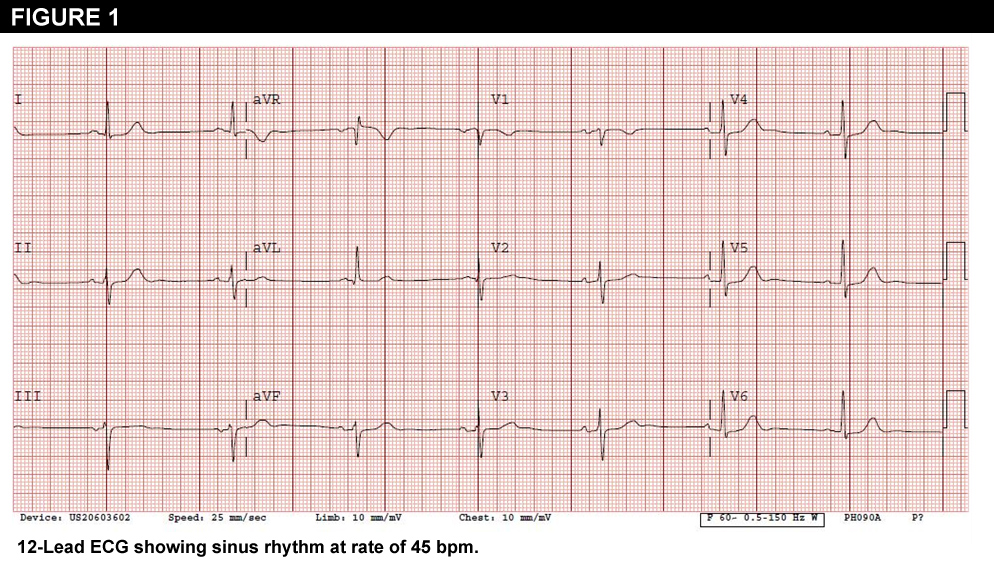
PEx: BP 124/74, P 45. CV: regular rhythm without murmurs Lungs: clear Ext: no edema with 2+ distal pulses
Labs: WNL (CBC and chemistry)
Echocardiogram: LV function is normal; no valvular abnormalities; LA size 4.0 cm
ECG: NSR (See Figure 1)
What is the next most appropriate step in the management of his atrial fibrillation?
Show Answer
The correct answer is: C. AF ablation (pulmonary vein isolation)
Two frequently asked questions are “whom to refer for ablation?” and “what do you ablate?”
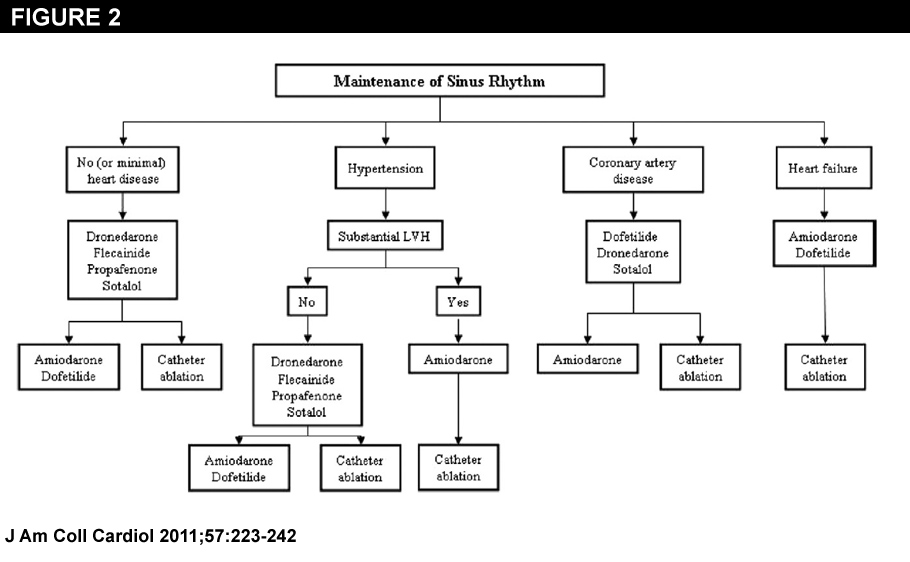
The recently updated Guidelines for Management of AF recommends ablation as an option for patients who do not respond to antiarrhythmic medication.(1) (Figure 2)
There are several features about this patient that make ablation an excellent option for him.
First, his episodes are paroxysmal. Most studies demonstrate higher ablation success rates in paroxysmal patients as compared to persistent or long-standing persistent AF.(2,3) Second, he has ‘lone’ AF (no concomitant heart disease) with a normal left atrial size. Again, success rates are higher in patients who have less structural heart disease.(4) Third, he continues to have symptomatic episodes despite antiarrhythmic drugs. Success rates in maintaining normal rhythm in patients who have failed antiarrhythmic drugs are higher with ablation as opposed to trying alternative antiarrhythmic medications.(5-7)
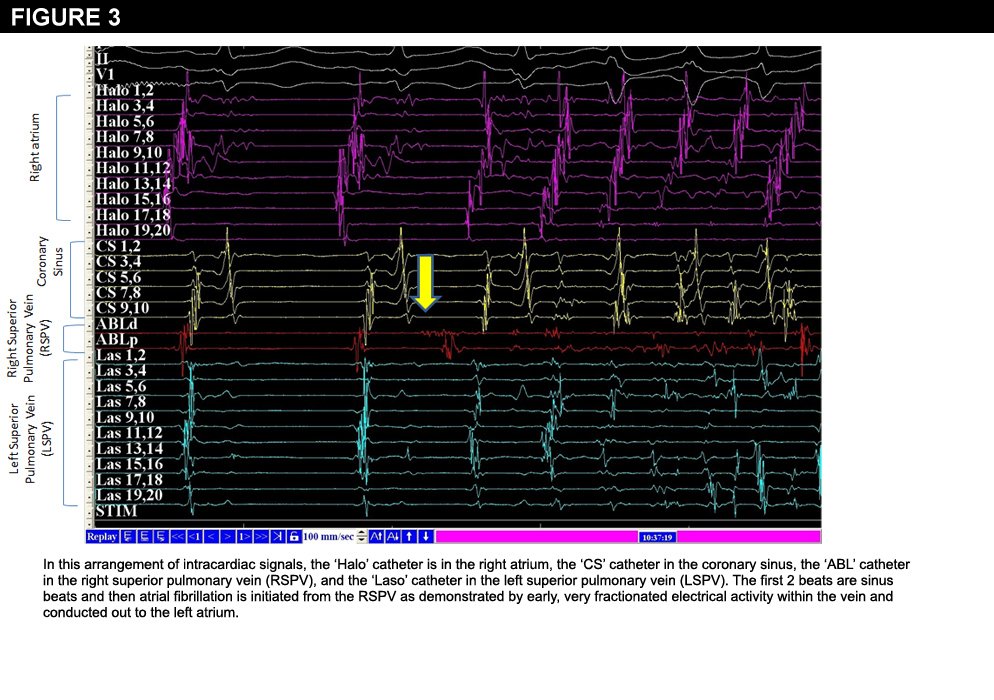
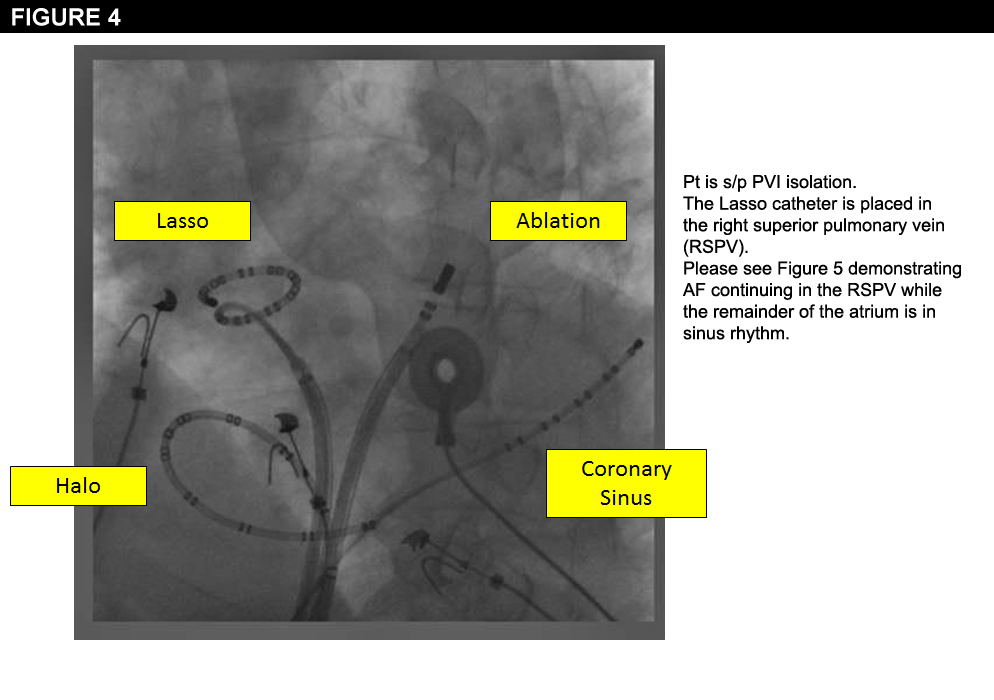
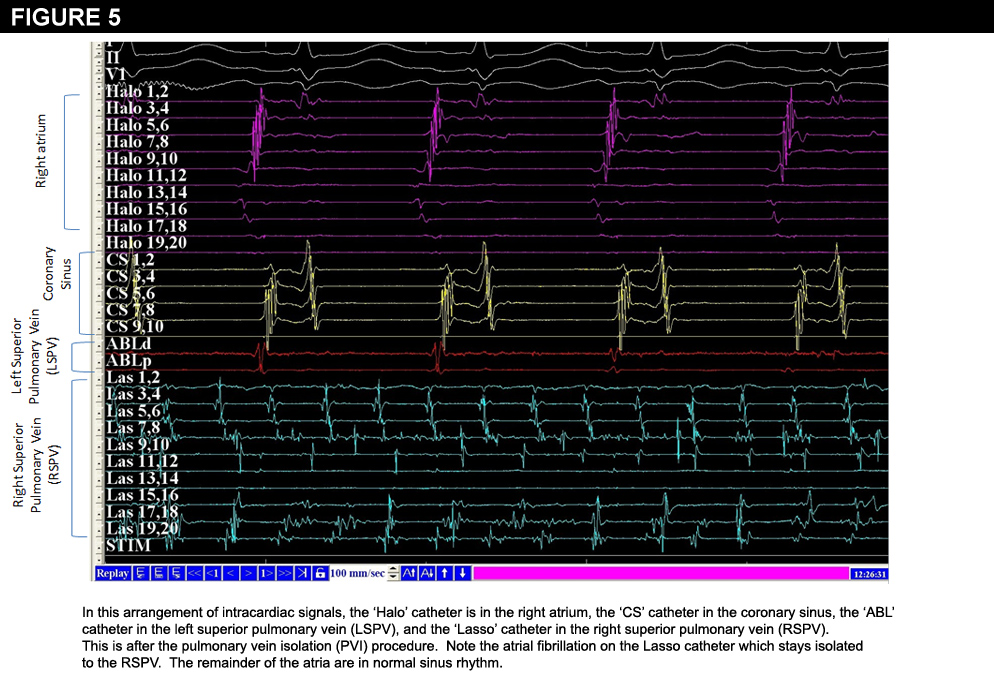
In the late 1990’s it was demonstrated that patients with paroxysmal AF may have triggers originating from the pulmonary vein (PV) area and that these can serve as arrhythmogenic foci.(8,9) The PVs’ are targeted for ablation for most patients with paroxysmal AF who undergo an AF ablation.(10) The endpoint is to electrically isolate the PV. This case shows a trigger (Figure 3) from the RSPV and nicely demonstrates isolation of the PV. (Figures 4 and 5). In patients who have more persistent AF or significant structural heart disease, additional ablation is frequently performed, but PV isolation remains the cornerstone of the procedure.
Usually, AVJ ablation + pacemaker insertion is reserved for those patients who have failed other attempts at rate/rhythm control with medications or catheter ablation of AF. In 2005 Hsieh, et al.(11) compared catheter ablation versus AVJ ablation + pacing in elderly patients with medically refractory paroxysmal AF (similar to our patient). They found that AVJ ablation + pacing was associated with a higher incidence of persistent AF and heart failure. Additionally, the PABA-CHF study compared AVJ ablation + bi-ventricular pacing versus catheter ablation in patients with drug-resistant AF, ejection fraction of 40% or less and NYHA CHF II or III. The composite primary endpoint (quality of life questionnaire, echocardiography, and 6-minute walk test) favored the group that underwent catheter ablation.(12)
ABL indicates ablation; AF, atrial fibrillation; AVJ, atrioventricular junction; CS, coronary sinus; LSPV, left superior pulmonary vein; PV, pulmonary vein; RSPV, right superior pulmonary vein.
References
Wann LS, Curtis AB, January CT et al. 2011 ACCF/AHA/HRS Focused Update on the Management of Patients with Atrial Fibrillation (Updating the 2006 Guideline). A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;57:223-242.
Fisher JD, Spinelli MA, Mookherjee D, et al. Atrial fibrillation: reaching the mainstream. PACE 2006;29:523-37.
Bhargava M, DiBiase L, Mohanty P, et al. Impact of type of atrial fibrillation and repeat catheterr ablation on long-term freedom from atrial fibrillation: results from a multicenter study. Heart Rhythm 2009;6:1403.
Hof I, Chilukur K, Arbab-zadeh A, et al. Does left atrial volume and pulmonary venous anatomy predict the outcome of catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2009;20:1005.
Teresawa T, Balk EM, Chung M, et al. Systematic review: comparative effectiveness of radiofrequency catheter ablation for atrial fibrillation. Ann Intern Med 2009;151:191.
Wilber DJ, Pappone C, Neuzil, P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized control trial. JAMA 2010;303:333.
Packer DL, Irwin JM, Champagne J, et al. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Artic Front STOP-AF pivotal trial. J Am Coll Cardiol 2010;55:E3015.
Jais P, Haissaguerre M, Shah D, et al. A Focal source of atrial fibrillation treated by discrete radiofrequency ablation. Circulation 1997;95:572.
Haissaguerre M, Jais P, Shah D, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659.
Calkins H, Burgada J, Packer DL, et al. HRS/EHRA/ECAS expert consensus statement on catheter ablation and surgical ablation of atrial fibrillation:recommendations for personnel, policy, procedures and follow-up. Heart Rhythm 2007;4:816.
Hsieh MH, Tai CT, Lee SH, et al. Catheter ablation of atrial fibrillation versus atrioventricular junction ablation plus pacing therapy for elderly patients with medically refractory paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol 2005;16:457.
Khan MN, Jais P, Cummings J, et al. Pulmonary-Vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med 2008;359:1778-85.