View other clinical content from the Bordeaux Group at:
A 68-year-old male patient who received an implantable cardioverter-defibrillator (ICD) cardiac resynchronization therapy (CRT) presented at an outpatient visit with progressive occurrence of shortness of breath. The internet reports provided by the home monitoring system did not identify any atrial or ventricular arrhythmia, or even any electrical shock.
This patient presents with a stable dilated cardiomyopathy (with wide QRS complexes and left ventricular ejection fraction [LVEF] assessed at 33% by echocardiogram) and documented episodes of ventricular tachycardia, underwent implantation of his ICD CRT two years ago and never presented with sustained ventricular arrhythmia. Physicians have just noticed that he has experienced several asymptomatic short salves of atrial arrhythmias.
During the outpatient visit, his echocardiogram shows worsening heart failure (LVEF at 29%) for the first time.
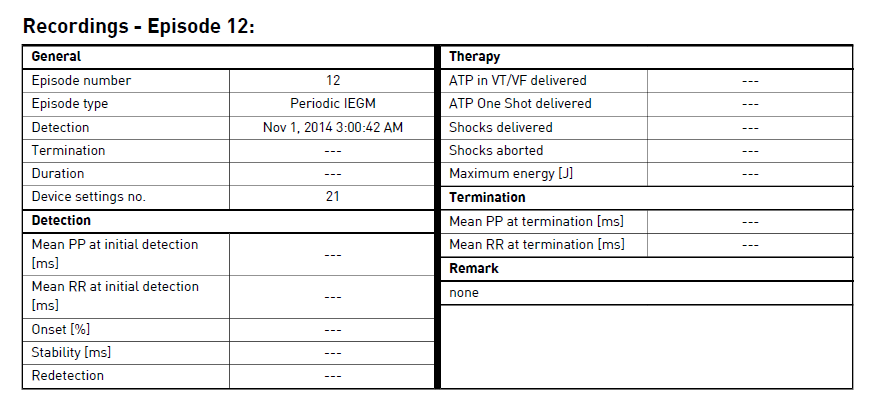
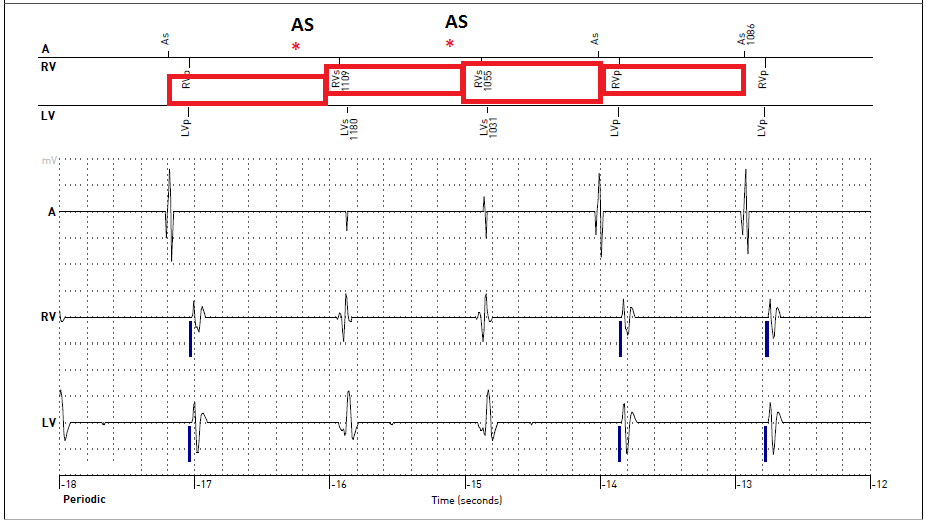
The memory function of the ICD is interrogated, and only a series of periodic intracardiac electrograms (IEGMs) are mentioned (Figures 1 and 2); this series is analyzed. Table 1 displays the analysis of the periodic IEGM #12.
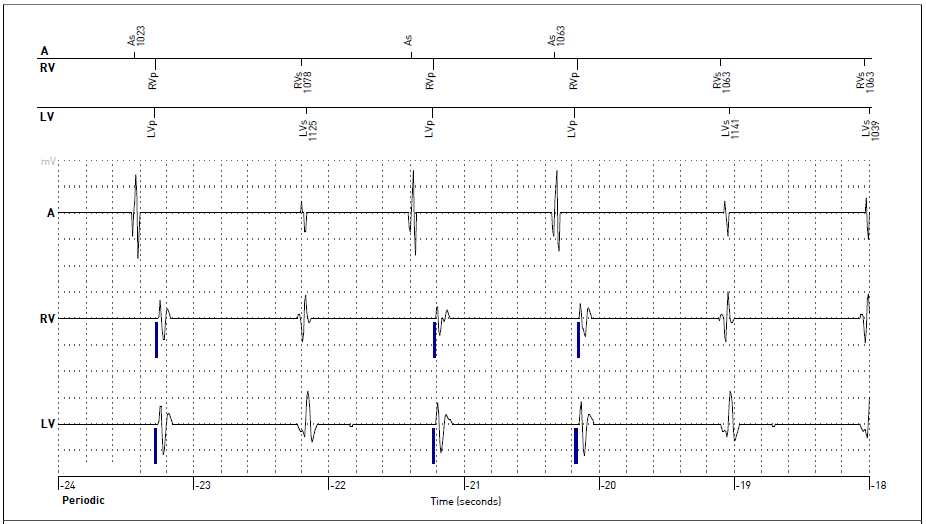
Figure 1
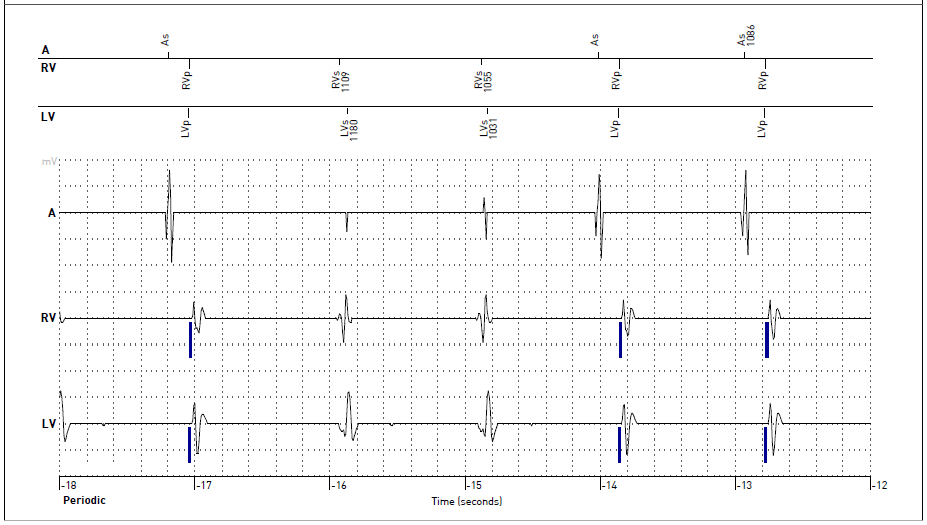
Figure 2
Table 1
Which of the following statements describes how one should interpret this tracing report from the home monitoring system?
Show Answer
The correct answer is: D. Loss of atrial sensing.
First, the text report of the periodic IEGM tracing does not display anything abnormal.
The tracings by themselves are crucial in order to understand what is going on in this particular situation. Indeed, the channel signals for this particular system are filtered; in other words, what you see on the screen are not the real signals. Accordingly, if there is no signal on a given channel (i.e., flat-line), it does not mean there is no signal; it just means this considered channel did not sense anything.
In Figures 1 and 2, we can notice three spontaneous QRS complexes (2nd, 5th, and 6th QRS complexes with no biventricular pacing). One could imagine frequent premature ventricular complexes. However, notice that the supposed coupling interval is close to the spontaneous sinus rhythm of the patient.
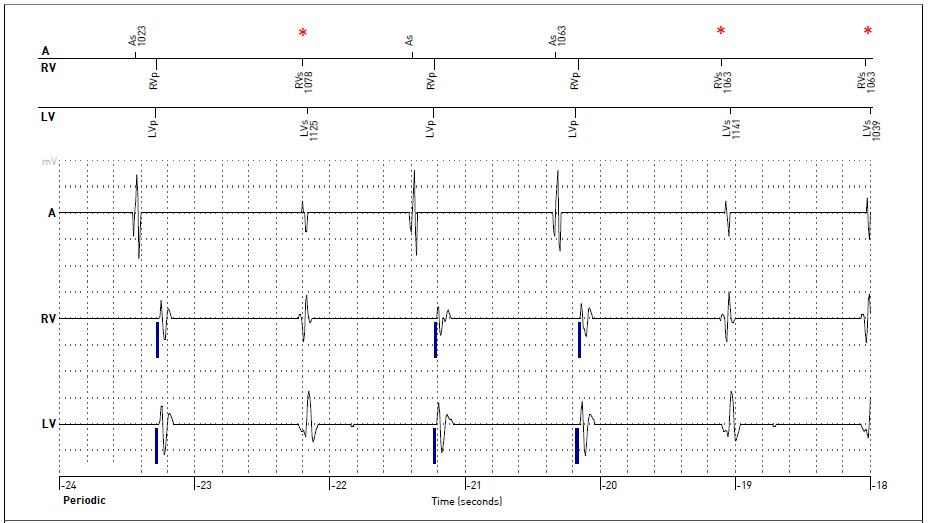
Consequently, one can assume that some atrial signals have not been sensed in a non-pacing-dependent patient; the supposed premature ventricular complexes are just the spontaneous ventricular complexes generated by the patient's sinus rhythm (Figures 3).
Figure 3
Then, answer option D is likely true for this tracing.
Figure 4 also highlights the similar time interval between two "AS" events identified by the atrial channel and the other supposed time intervals if answer option D is correct.
Figure 4
The atrial sensing was programmed to 1 mV; it was modified down to 0.5 for a sensing threshold reaching 1.3 mV.
Notice that the other periodic IEGM tracings of this patient showed similar features. Two weeks after this ICD reprogramming, all clinical symptoms disappeared.
This case highlights the potential risks associated with non-interpretation of periodic IEGM tracings in home monitoring systems. Indeed, we would usually (and incorrectly) rather focus on events registered and stored by the memory function but not very much on periodic tracings.
References
Jastrzebski M, Kukla P, Fijorek K, Czarnecka D. Universal algorithm for diagnosis of biventricular capture in patients with cardiac resynchronization therapy. Pacing Clin Electrophysiol 2014;37:986-93.
Steffel J, Hürlimann D. An unusual reason for loss of biventricular pacing. Pacing Clin Electrophysiol 2014;37:383-6.
Barold SS, Kucher A. Understanding the timing cycles of a cardiac resynchronization device designed with left ventricular sensing. Pacing Clin Electrophysiol 2014;37:1324-37.