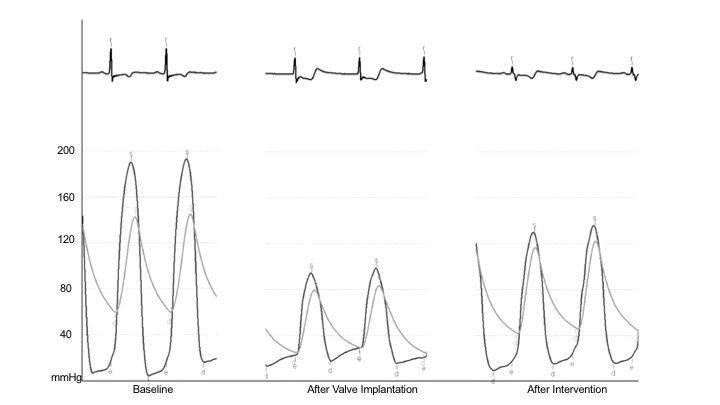
A 76-year-old female patient with a prior history of coronary artery bypass surgery, chronic kidney disease, and chronic obstructive lung disease presented with exertional shortness of breath on minimal activity such as going up a flight of stairs. Coronary and graft angiography revealed patent right and left circumflex coronary arteries and grafts (left internal mammary graft to the left anterior descending artery and a saphenous vein graft to a diagonal artery). Transthoracic echocardiography showed severe aortic stenosis and preserved left ventricular (LV) systolic function. She was considered high risk for surgical aortic valve replacement, and it was elected to replace her aortic valve using a transcatheter approach. Cardiac computed tomography evaluation of the aortic annulus indicated that a 26 mm CoreValve Evolut R (Medtronic, Inc.; Minneapolis, MN) self-expanding transcatheter heart valve would be appropriate with 16% oversizing. Transcatheter aortic valve replacement (TAVR) using a 26 mm CoreValve Evolut R (Medtronic, Inc.; Minneapolis, MN) valve was performed from the right femoral approach under conscious sedation. Immediately following valve deployment, the patient was noted to be hypotensive. Left ventricular-aortic simultaneous pressure tracings are shown at baseline, following valve deployment and after a subsequent percutaneous intervention (Figure 1). Ascending aortic angiography is also shown immediately following valve deployment (Video 1).
Figure 1
Video 1
What was the cause of the patient's hemodynamic decompensation, and what acute intervention was performed?
Show Answer
The correct answer is: B. Severe acute aortic peri-prosthetic regurgitation treated with prosthetic balloon post-dilatation
Intraprocedural circulatory depression with cardiogenic shock may occur during TAVR. The differential diagnosis for acute hemodynamic compromise following TAVR includes ischemia secondary to coronary ostial occlusion, severe acute prosthetic or peri-prosthetic regurgitation, pericardial tamponade due to aortic root rupture, LV perforation from guide-wires, right ventricular perforation from pacing wires, and severe bradycardia due to conduction system abnormalities.
In this case, there was a rapid rise in LV diastolic pressure and equalization of LV end-diastolic and aortic diastolic pressures that was concerning for acute severe prosthetic or peri-prosthetic regurgitation. Ascending aortic angiography in this case confirmed that peri-prosthetic regurgitation (answer B) was the cause for the acute hemodynamic changes. Acute prosthetic (answer A) or peri-prosthetic regurgitation is not accompanied by LV remodelling and dilatation seen in chronic regurgitation that is needed to augment stroke volume and increase forward flow. A stiff, non-compliant LV (due to age and aortic stenosis) results in the rapid rise of LV diastolic pressure, causing diastasis to occur earlier in diastole. Acute peri-prosthetic regurgitation following TAVR with the self-expanding CoreValve Evolut R (Medtronic, Inc.; Minneapolis, MN) valve may be due to a low implantation height. A valve implanted more than 12 mm below the annulus may result in valve frame cells that are not covered by the extended sealing skirt being positioned below the annulus. Angiography in this case showed that valve implantation height was correct within the recommended 4-6 mm range. Peri-prosthetic regurgitation in a valve implanted at the correct height is generally due to valve underexpansion within a severely calcified aortic valve or underestimation of aortic annulus measurement. Careful computed tomography measurements were performed in this case to ensure appropriate valve size selection, and the valve implanted was 16% oversized. The most likely cause was likely an underexpanded valve related to severe calcification that was successfully treated with prosthetic balloon post-dilatation, resulting in rapid recovery of patient's blood pressure. Only mild residual peri-prosthetic regurgitation was seen in the transthoracic echocardiogram 1 day post-operation.
Although telemetry showed ST-segment depression, ascending angiography confirmed patent flow in the ungrafted right coronary artery as well as diagonal vein graft, making it less likely that coronary ischemia (answer C) was the cause for hypotension. The patient was known to have a patent left internal mammary artery to left anterior descending that was unlikely to have been affected during TAVR from a transfemoral approach. Unchanged heart borders on fluoroscopy and LV-aortic pressure waveforms without significant respiratory variation (pulsus paradoxus) make pericardial tamponade (answer D) a less-likely etiology for hypotension. A transthoracic echocardiogram performed following prosthetic balloon post-dilatation did not show pericardial effusion. Telemetry immediately following valve deployment shows a junctional rhythm without bradycardia (answer E). A junctional rhythm is associated with loss of the contribution of atrial systole to LV diastolic filling, but it is unlikely to explain the changes in the LV-aortic pressure waveforms noted as well as the aortic root angiography findings.
References
Serruys PW, Piazza N, Cribier A, Webb JG, Laborde JC, dr Jargere P. Transcatheter Aortic Valve Implantation: Tips and Tricks to Avoid Failure. New York: Informa Healthcare; 2010.
Ragosta M. Textbook of Clinical Hemodynamics. 1st ed. Philadelphia: Saunders Elsevier; 2008.
Eisenhauer MD, Kern MJ. Invasive Hemodynamics in the Catheterization Laboratory: Self-Assessment and Review. 1st ed. London: Remedica Publishing; 2002.