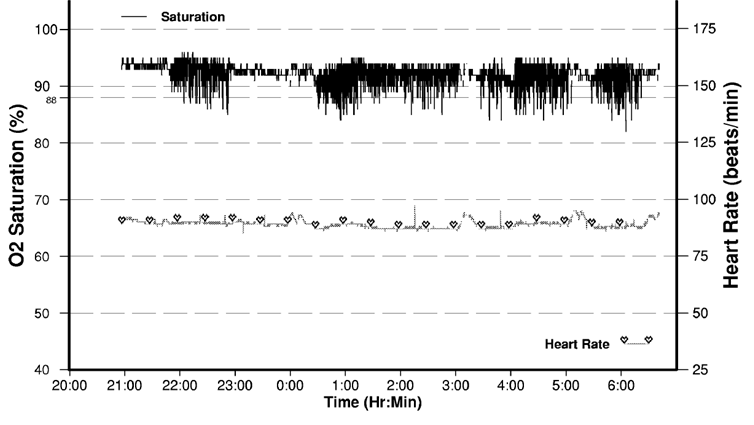
A 67-year-old man presents with a three-month history of pauses in breathing during sleep, witnessed by his wife. There is no history of snoring or difficulty falling asleep, although he has been waking up occasionally due to shortness of breath which resolves several minutes after sitting upright. He has recently been diagnosed with heart failure and his medications are aspirin, lisinopril, atorvastatin, and metoprolol. Vitals: temperature 36.6 °C (97.9 °F), left arm BP 128/78 mm Hg, pulse rate 88/min, respiration rate 16/min, body mass index 24 kg/m2. Cardiorespiratory examination demonstrates regular pulse, an S3 without any murmurs, JVP 6 cm, bibasilar crackles and trace bipedal edema. Overnight sleep oximetry reveals baseline saturations of 94% on room air with frequent desaturations (Figure 1). On polysomnography, there is characteristic Cheyne-Stokes ventilation.
Figure 1: Overnight Sleep Oximetry at Presentation
Which of the following is the next best therapeutic intervention for this patient?
Show Answer
The correct answer is: C. Diuretic therapy.
The patient's presentation is classic for central sleep apnea (CSA). As opposed to obstructive sleep apnea (OSA), which is caused by pharyngeal collapse and reduced airflow during sleep despite ongoing respiratory effort, CSA is caused by cyclic loss of central respiratory drive resulting in crescendo-decrescendo ventilation and periodic apnea (Cheyne-Stokes breathing).1-3 Although the pathophysiology is not fully understood, it is strongly associated with heart failure; other risk factors include stroke and advanced age. Table 1 summarizes the clinical features, investigative workup, and therapeutic strategies for CSA and OSA. Distinguishing between the two is important because of the difference in etiology and management. Overnight oximetry has been used as a screening tool, though is not reliable in heart failure patients for this purpose.4 If CSA is suspected, multi-channel overnight polysomnography is recommended.2
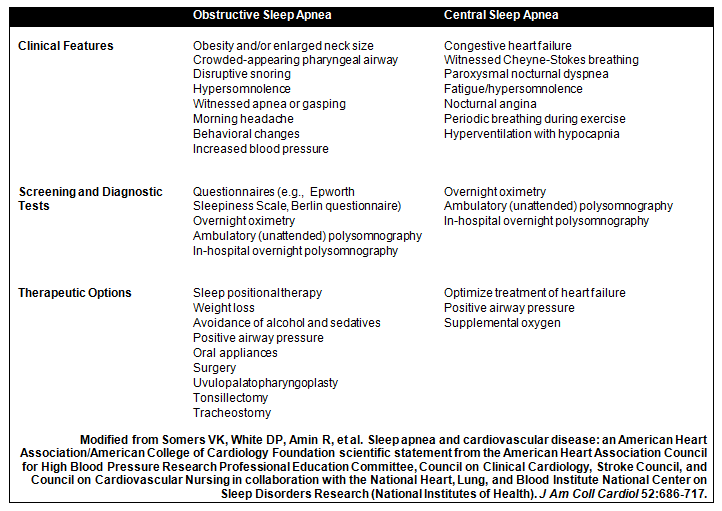
Table 1: Obstructive vs. Central Sleep Apnea: Clinical Features, Investigations, and Therapy
Figure 1: Overnight Sleep Oximetry at Presentation
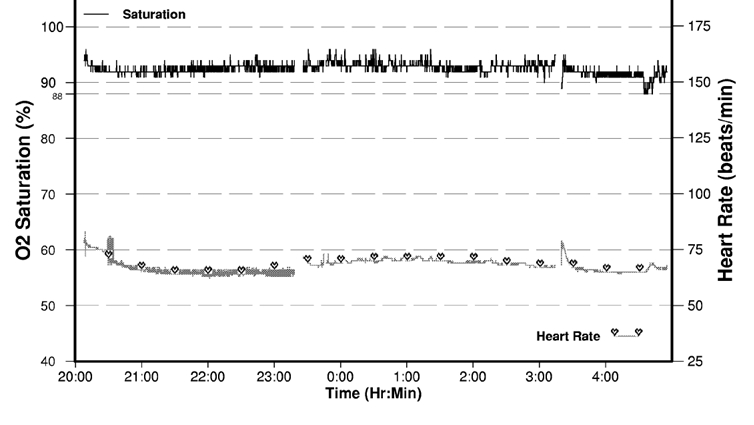
Figure 2: Overnight Sleep Oximetry After Diuretic Therapy
This patient has CSA related to heart failure. In heart failure patients, reduced diffusing capacity, often related to pulmonary edema is a factor in the pathogenesis of CSA.5 Optimizing medical therapy of heart failure is the first step in management. Therefore, the correct answer in this patient, who is clinically fluid overloaded, is institution of diuretic therapy. Figure 2 demonstrates the nearly normal repeat overnight sleep oximetry after adequate diuretic therapy.
Some patients with persistent CSA may require positive airway pressure (PAP) therapy.2,5 Continuous positive airways pressure (CPAP) may be effective in some cases, particularly in those with a mixed obstructive apnea component. The emerging PAP device of choice in central sleep apnea syndromes is probably adaptive servoventilation (ASV) which synchronizes ventilation with the patient's variable breathing effort.2 Although these therapies have been shown to reduce CSA severity, there is limited evidence that important cardiovascular outcomes are altered. Large clinical studies of ASV in CSA designed to provide these answers are ongoing. Supplemental nocturnal oxygen can also be considered for select cases as second line, and although theophylline may also reduce CSA severity, it is not recommended due to its proarrhythmic effects.2
References
Caples SM, Wolk R, Somers VK. Influence of cardiac function and failure on sleep-disordered breathing: evidence for a causative role. J Appl Physiol 2005;99:2433-9.
Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation scientific statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing in collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health). J Am Coll Cardiol 52:686-717.
Szollosi I, Thompson BR, Krum H, et al. Impaired pulmonary diffusing capacity and hypoxia in heart failure correlates with central sleep apnea severity. Chest 2008 134:67-72.
Sériès F, Kimoff RJ, Morrison D, et al. Prospective evaluation of nocturnal oximetry for detection of sleep-related breathing disturbances in patients with chronic heart failure. Chest 2005;127:1507-14.
Olson LJ, Somers VK. Treating central sleep apnea in heart failure: outcomes revisited. Circulation 2007;115: 3140-2.