A 57-year-old Caucasian man presents to the cardiology clinic complaining of worsening symptoms of dyspnea on exertion and fatigue for the last six weeks. He has a history of insulin-dependent diabetes mellitus, hypertension (HTN), and dyslipidemia. There is no history of tobacco or alcohol use. Family history is significant for diabetes mellitus and HTN in both parents as well as fatal coronary artery disease (CAD) in his father.
He is married, works in the library of the local university, and spends a great amount of time sitting at a desk. He tries to be sensible about his diet, but does admit that his "diabetes has not been under the best control." He does not participate in any regular exercise, but was able to walk up two flights of stairs without difficulty until the last six weeks. On exam, blood pressure is 157/85 mm Hg, body mass index (BMI) 29 kg/m2, and waist circumference 118 cm. The rest of the physical examination is normal. The laboratory studies show total cholesterol of 230mg/dL, high-density lipoprotein cholesterol (HDL-C) 28 mg/dL, triglycerides 158 mg/dL, and HbA1c 7.9%.
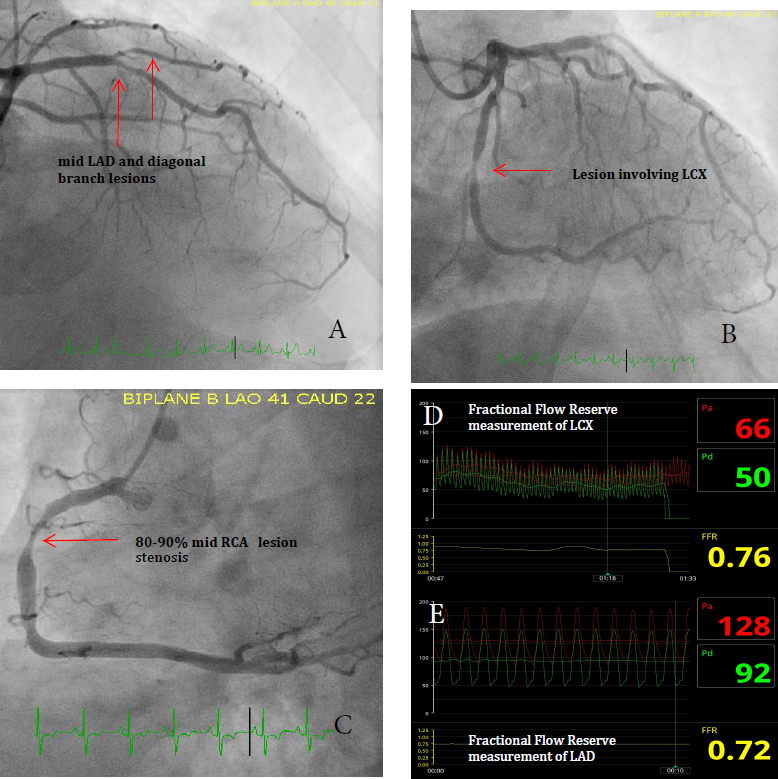
Given his symptoms, the patient undergoes a nuclear myocardial perfusion stress testing. The study reveals a moderate area of inferior ischemia and mild distal anterior and apical ischemia. He subsequently undergoes cardiac catheterization. His coronary angiogram reveals 80-90% mid right coronary artery (RCA) stenosis, 50-70% proximal left circumflex (LCX) stenosis, and 50-70% stenosis of the mid left anterior descending coronary artery (LAD) and diagonal branch. Given the possibility of significant LAD and LCX disease, fractional flow reserve (FFR) measurements are performed on the LAD and LCX. Fractional flow reserve (FFR) of the LAD is 0.72, and LCX is 0.76 (anything less then 0.80 is felt to be physiologically significant). This suggests that he has significant three-vessel CAD involving the RCA, LAD, LCX (Figure 1). However, all lesions are angiographically focal in appearance (and without significant tortuosity or calcification), and his calculated SYNTAX score is approximately 16.1 The cumulative four-year major adverse cardiac and cerebrovascular event rate (MACCE) rate for this SYNTAX score is approximately 28% for coronary artery bypass graft (CABG) or percutaneous coronary intervention (PCI) (score for all patients and not specifically for patients with diabetes) for revascularization via either coronary artery bypass graft surgery (CABG) or percutaneous coronary intervention (PCI). For patients with three-vessel CAD and SYNTAX scores ≥33 the five year data2 suggests MACCE rates that range from 27% for CABG versus 44% for PCI (p <0.001).
Figure 1
LAD = left anterior descending coronary artery; LCX – proximal left circumflex; RCA = right coronary artery.
The SYNTAX score was developed to prospectively characterize the coronary vasculature with respect to the number of lesions and their anatomical complexity, location and functional impact. Lower SYNTAX scores (less than 22) are indicative of less complex disease and are thought to represent less revascularization challenges and, therefore, may give rise to better prognosis. High SYNTAX scores may represent more complex lesion anatomy. These lesions provide greater technical challenges during PCI and, consequently, a higher risk of adverse events. CABG surgery bypasses the lesion and is less influenced by the complexity of lesions. Therefore, CABG may be more ideal for patients with high SYNTAX scores.
Given this information, it can be difficult deciding on the most optimal revascularization strategy for such diabetic patients with three-vessel CAD and low SYNTAX scores.
In the context of such risk stratification, which of the following statements is FALSE and should not be part of your patient evaluation?
Show Answer
The correct answer is: E. The FREEDOM trial suggested that CABG was NOT superior to PCI with drug-eluting stents in patients with diabetes and multivessel CAD because CABG did not significantly reduce rates of death and myocardial infarction (MI).
Answer option A is true. Diabetes mellitus is a major risk factor for premature and aggressive CAD. This may be due to the presence of endothelial dysfunction, greater amount of thrombotic and inflammatory cytokines in this population, and the greater degree of insulin resistance and oxidative stress in these patients. All can lead to more aggressive and premature atherosclerosis in patients with diabetes.3-8
Answer option B is true. Studies have suggested that diabetics who have CABG have higher incidence of postoperative renal impairment, neurological complications and of postoperative infection.9-11 Diabetic patients who undergo PCI also have higher rates of coronary stent thrombosis and restenosis.12,13
Answer option C is true. The SYNTAX score is an angiographic grading tool to determine the complexity of CAD. The score was derived from other pre-existing classifications.14,15 However, this score does consider the clinical features of the patient.
As a result of this, the "Clinical SYNTAX score" was developed. This tool incorporates clinical features such as age, ejection fraction, and renal function with the anatomic angiographic assessment.16-18 The Clinical SYNTAX score has shown better ability to predict major adverse cardiac events and mortality compared with the anatomic SYNTAX score. Additionally, a "functional SYNTAX score" incorporates the use of intravascular physiology by FFR for better risk stratification of patients.19 The integration of FFR and SYNTAX showed better predictions of clinical outcome than just the anatomic SYNTAX score.
Answer option D is true. The Synergy Between Percutaneous Coronary Intervention With TAXUS and Cardiac Surgery (SYNTAX) trial compared PCI with paclitaxel-eluting stents (PES) and CABG for patients with de novo three-vessel and/or left main disease.20,21 Subgroup analyses of diabetic versus non-diabetic patients examined the impact of diabetes on outcomes after up to five years after PCI and CABG.22,23
Patients (n = 1800) with Left Main and/or three-vessel CAD were randomized to receive either PCI with TAXUS Express paclitaxel-eluting stents or CABG. Five-year outcomes in subgroups with (n = 452) or without (n = 1,348) diabetes were examined.
The rate of MACCE was significantly higher in patients with PCI compared with CABG (37% versus 27%, respectively; P <0.001).
PCI compared to CABG resulted in significantly higher rates of the composite of death/stroke/MI (22.0 vs. 14.0%, respectively; P <0.001), all-cause death (14.6 vs. 9.2%, respectively; P = 0.006), MI (9.2 versus 4.0%, respectively; P = 0.001), and repeat revascularization (13.7% versus 25.9%; p <0.0001).
Results (for the overall sample group) were dependent on lesion complexity. Patients with a low (0-22) SYNTAX score had similar rates of MACCE for PCI versus CABG (33.3% vs. 26.8%, respectively; P = 0.21), but significantly more repeat revascularization (25.4% vs. 12.6%, respectively; P = 0.038). In intermediate (23-32) or high (≥33) SYNTAX score groups, CABG demonstrated superiority in terms of MACCE, death, MI, and repeat revascularization. Differences in MACCE between PCI and CABG were larger in diabetics [hazard ratio (HR) = 2.30] than non-diabetics (HR = 1.51), although P was not significance for MACCE (P for interaction = 0.095) for any of the other endpoints.
The study suggested that although PCI is a potential treatment option in patients with less-complex lesions, CABG should be the revascularization choice for patients with more-complex anatomic disease, especially diabetic patients.24
Answer option E is false and, therefore, the correct answer. FREEDOM trial (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) evaluated whether PCI with drug-eluting stents was more or less effective than the CABG in patients with diabetes mellitus.11 The study enrolled 1,900 adults with diabetes mellitus (type 1 or type 2) with angiographic multivessel CAD. The participants were randomly assigned to receive one of the interventions. PCI was with sirolimus-eluting and paclitaxel-eluting stents. Dual antiplatelet therapy was recommended for at least 12 months, and patients were followed for a minimum of two years.
The study found that there was increased all-cause mortality in the PCI group (16.3% in the PCI group vs. 10.9% in the CABG group) at the end of a five-year period. It was also seen that 13.9% of patients in the PCI group had an MI, as compared with 6% in the CABG group. However, there were fewer strokes in the PCI group (2.4%) than in the CABG group (5.2%). There was also a significant difference in rates of MACCE at one year after the procedure, with 16.8% in the PCI group versus 11.8% in the CABG group suffering from these adverse events. Based on the results of the trial, it was concluded that CABG was superior to PCI with drug-eluting stents in patients with diabetes and multivessel CAD as CABG significantly reduced rates of death and MI. However, it was associated with a higher rate of stroke.
References
van Gameren M. SYNTAX Score (SYNTAX Score Working Group website). 2009-2013. Available at: http://syntaxscore.com. Accessed 1/26/2015.
Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet 2013;381:629-38.
Lincoff AM. Important triad in cardiovascular medicine: diabetes, coronary intervention, and platelet glycoprotein IIb/IIIa receptor blockade. Circulation 2003;107:1556-9.
Aronson D, Bloomgarden Z, Rayfield EJ. Potential mechanisms promoting restenosis in diabetic patients. J Am Coll Cardiol 1996;27:528-35.
Moreno PR, Murcia AM, Palacios IF, et al. Coronary composition and macrophage infiltration in atherectomy specimens from patients with diabetes mellitus. Circulation 2000;102:2180-4.
Bluher M, Unger R, Rassoul F, et al. Relation between glycaemic control, hyperinsulinaemia and plasma concentrations of soluble adhesion molecules in patients with impaired glucose tolerance or type II diabetes. Diabetologia 2002;45:210-6.
Creager MA, Luscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Circulation 2003;108:1527-32.
Biondi-Zoccai GG, Abbate A, Liuzzo G, Biasucci LM. Atherothrombosis, inflammation, and diabetes. J Am Coll Cardiol 2003;41:1071-7.
Morricone L, Ranucci M, Denti S, et al. Diabetes and complications after cardiac surgery: comparison with a non-diabetic population. Acta Diabetol 1999; 36:77-84.
Hogue CW Jr., Murphy SF, Schechtman KB, Davila-Roman VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation 1999;100:642-7.
Farkouh ME, Domanski M, Sleeper LA, et al; FREEDOM Trial Investigators. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med 2012;367:2375-84.
Mathew V, Gersh BJ, Williams BA, et al. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era: a report from the Prevention of REStenosis with Tranilast and its Outcomes (PRESTO) trial. Circulation 2004; 109:476–80.
Glaser R, Selzer F, Faxon DP, et al. Clinical progression of incidental, asymptomatic lesions discovered during culprit vessel coronary intervention. Circulation 2005;111:143-9.
Serruys PW, Onuma Y, Garg S, et al. Assessment of the SYNTAX scores in the syntax study. EuroIntervention 2009;5: 50-6.
Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention 2005;1:219-27.
Capodanno D, Miano M, Cincotta G, et al. Euroscore refines the predictive ability of SYNTAX score in patients undergoing left main percutaneous coronary intervention. Am Heart J 2010;159:103–9.
Capodanno D, Caggegi A, Miano M, et al. Global risk classification and clinical SYNTAX (synergy between percutaneous coronary intervention with taxus and cardiac surgery) score in patients undergoing percutaneous or surgical left main revascularization. JACC Cardiovasc Interv ;2011;4:287-97.
Girasis C, Garg S, Raber L, et al. Syntax score and clinical SYNTAX score as predictors of very long-term clinical outcomes in patients undergoing percutaneous coronary interventions: a substudy of sirolimus-eluting stent compared with paclitaxel-eluting stent for coronary revascularization (SIRTAX) trial Eur Heart J 2011;32:3115-27.
Nam CW, Mangiacapra F, Entjes R, et al. Functional SYNTAX score for risk assessment in multivessel coronary artery disease. J Am Coll Cardiol 2011;58:1211-8.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med 2009;360:961-72.
Kappetein AP, Feldman TE, Mack MJ, et al. Comparison of coronary bypass surgery with drug-eluting stenting for the treatment of left main and/or three-vessel disease: 3-year follow-up of the SYNTAX trial. Eur Heart J 2011;32:2125-34.
Banning AP, Westaby S, Morice M-C, et al. Diabetic and nondiabetic patients with left main and/or 3-vessel coronary artery disease: comparison of outcomes with cardiac surgery and paclitaxel-eluting stents. J Am Coll Cardiol 2010;55:1067-75.
Mack MJ, Banning AP, Serruys PW, et al. Bypass versus drug-eluting stents at three years in SYNTAX patients with diabetes mellitus or metabolic syndrome. Ann Thorac Surg 2011;92:2140-6.
Kappetein AP, Head SJ, Morice MC, et al. Treatment of complex coronary artery disease in patients with diabetes: 5-year results comparing outcomes of bypass surgery and percutaneous coronary intervention in the SYNTAX trial. Eur J Cardiothorac Surg 2013;43:1006-13.