A 52-year-old male with drug-refractory and highly symptomatic paroxysmal atrial fibrillation was brought to the electrophysiology laboratory for a first attempt at ablation of his atrial fibrillation. A pre-operative CT scan confirmed the presence of four pulmonary veins with separate ostia.
A decapolar spiral mapping catheter and irrigated ablation catheter were each introduced into the left atrium (LA) via transseptal puncture. A further steerable decapolar catheter was placed in the coronary sinus (CS).
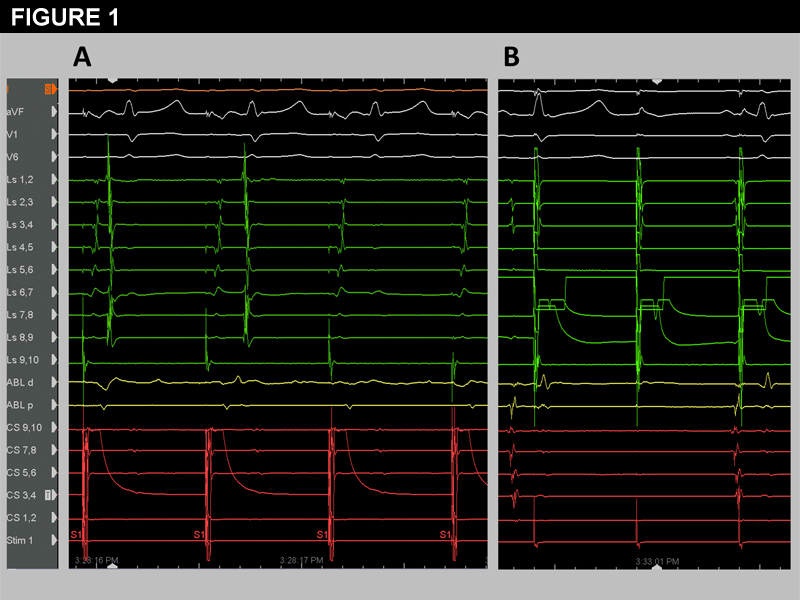
The left pulmonary veins were isolated as a common unit with a circumferential lesion set. Entrance block into the left superior pulmonary vein (LSPV) with ablation is demonstrated in Figure 1a with loss of the pulmonary vein electrograms (EGMs) on the spiral catheter (denoted as Ls). Note that ablation was performed during pacing from the distal CS catheter to better localize the remaining connection between the LA and the LSPV.
Exit block of the LSPV was then confirmed with high output (10 mA, 2.0ms) pacing around the spiral catheter (representative pacing from Ls 6,7 is shown in Figure 1b). The left inferior pulmonary vein was also confirmed to be isolated (entrance and exit block) with the same lesion set.
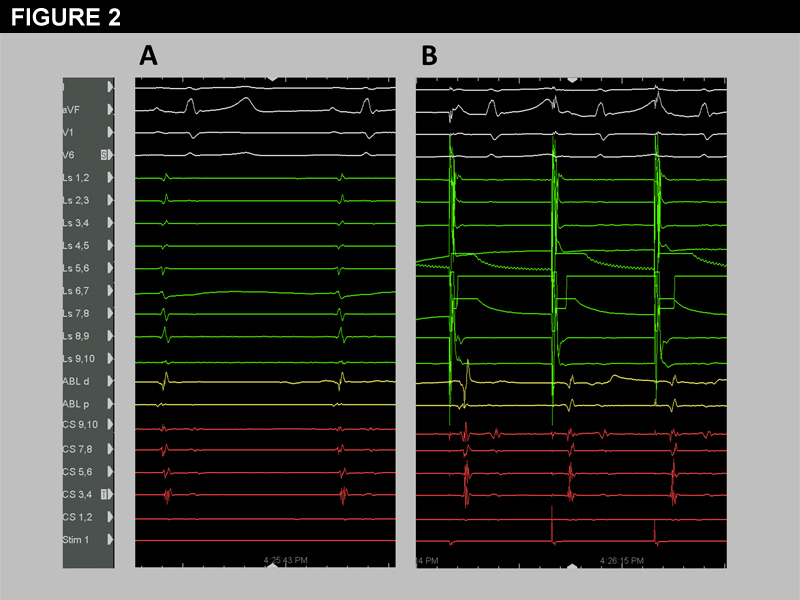
After subsequent isolation of the right pulmonary veins, the spiral catheter was replaced in the LSPV to assess for acute reconnection. Although the LSPV EGMs remained largely unchanged (Figure 2a), high output pacing (10mA, 2.0ms) from electrodes on the anterior margin of the vein now captured the LA, shown in Figure 2b. No spontaneous pulmonary vein potentials were seen in the LSPV.
The differential diagnosis for LA capture after apparent successful isolation of the LSPV includes: 1) subtle or unidirectional acute reconnection, 2) far-field capture of the left atrial appendage or 3) connection of the left pulmonary veins to the LA via the ligament of Marshall.
What is the appropriate next step in assessing the LSPV?
Show Answer
The correct answer is: D. Pace from the spiral catheter but at varying pacing outputs
Isoproterenol infusion may provoke spontaneous pulmonary vein firing in previously silent veins.1 The observance of spontaneous pulmonary vein firing without conduction to the LA is strong evidence that exit block from the vein persists, though it is not definitive. Unfortunately, a significant proportion of patients have no demonstrable firing in the pulmonary veins in question despite high-dose isoproterenol. High dose isoproterenol (20-40 mcg/minute) requires invasive hemodynamic monitoring and frequently requires concomitant vasopressor support.
Figure 1
Unidirectional pulmonary vein reconnection (entrance block but documented pulmonary vein to LA conduction) has been reported to occur prior to manifest bidirectional pulmonary vein reconnection.2 The administration of adenosine may therefore be useful if recurrent conduction from the left atrium to the pulmonary vein is demonstrated. Unfortunately again, such dormant reconnection is demonstrated only in 25% of pulmonary veins after initial successful isolation.3 Therefore the lack of manifest reconnection with adenosine would place us no further ahead.
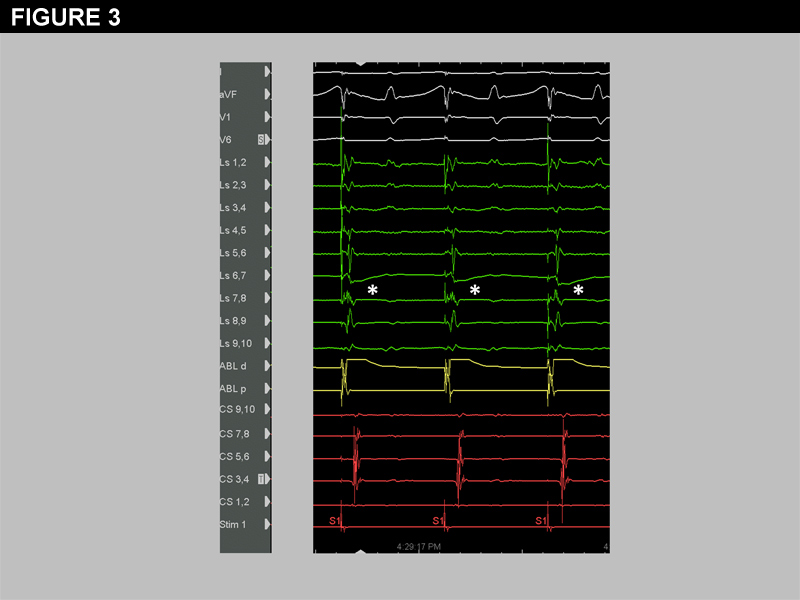
Pacing from the left atrial appendage using the ablation catheter is an excellent method of distinguishing far-field appendage signals from intrinsic pulmonary vein EGMs, to confirm entrance block.4 With left atrial appendage pacing any far-field signals from the appendage should be brought into or occur very shortly after the pacing stimulus. Pulmonary vein potentials, on the other hand, should be markedly delayed from the pacing stimulus after ablation around the majority of the circumference of the left pulmonary veins. Left atrial appendage pacing can be difficult to interpret after loss of the majority of pulmonary vein EGMs. In our case, the remaining potentials seen on the spiral catheter were not entirely brought into the stimulus (Figure 3) and the fractionated nature of the electrograms (especially on Ls 7,8 -denoted by the asterisks) gave us uncertainty about whether these were truly only far-field signals. Left atrial appendage pacing is a useful maneuver to confirm entrance block, but again provides us with no information on whether exit block is present. Therefore its utility in this case is minimal.
Alteration of the pacing output is an extremely useful maneuver by virtue of its ability to demonstrate differential capture of the pulmonary vein sleeve and far-field structures (such as the left atrial appendage). This is the most useful maneuver in this situation. Furthermore, this maneuver is also useful in distinguishing reconnection of the right superior pulmonary vein from far-field capture of the right atrium/superior vena cava with high output pacing.5Figure 4a demonstrates simultaneous capture of both the left atrial appendage and the pulmonary vein sleeve for the first two beats, while pacing from Ls 6,7 (located on the anterior aspect of the LSPV ostium). Decreasing the pacing output from 5 to 4mA resulted in loss of capture of the LA but persistent LSPV sleeve capture (the last two beats in Figure 4a). The LSPV sleeve capture may be subtle and is more apparent at a paper speed of 200 mm/s (Figure 4b, arrows). The ablation catheter may also be placed in the LA appendage (not shown) to confirm when loss of appendage capture occurs, though this is usually evident from the CS EGMs.
Demonstration of capture of the pulmonary vein sleeve without conduction to the left atrium, at multiple pacing rates, conclusively proves exit block from that pulmonary vein. This maneuver does not depend on the presence of spontaneous pulmonary vein firing, does not require introduction of extra catheters or the administration of additional intravenous drugs.>
References
Valles E, Fan R, Roux JF et al. Localization of atrial fibrillation triggers in patients undergoing pulmonary vein isolation: importance of the carina region. J Am Coll Cardiol 2008;52:1413-20.
Tritto M, De Ponti R, Salerno-Uriarte JA et al. Adenosine restores atrio-venous conduction after apparently successful ostial isolation of the pulmonary veins. Eur Heart J 2004;25:2155-63.
Arentz T, Macle L, Kalusche D et al. "Dormant" pulmonary vein conduction revealed by adenosine after ostial radiofrequency catheter ablation. J Cardiovasc Electrophysiol 2004;15:1041-7.
Shah D, Haissaguerre M, Jais P et al. Left atrial appendage activity masquerading as pulmonary vein potentials. Circulation 2002;105:2821-5.
Shah D, Burri H, Sunthorn H, Gentil-Baron P. Identifying far-field superior vena cava potentials within the right superior pulmonary vein. Heart Rhythm 2006;3:898-902.