A 61-year-old man presents to the emergency department with several days of palpitations and dyspnea. His past medical history is remarkable for an atrial fibrillation ablation three years ago, hypertension, hyperlipidemia, and obesity. Echocardiogram revealed normal left ventricle and right ventricle size and systolic function, with no significant valvular abnormalities.
A 12 lead ECG was obtained (Figure 1).
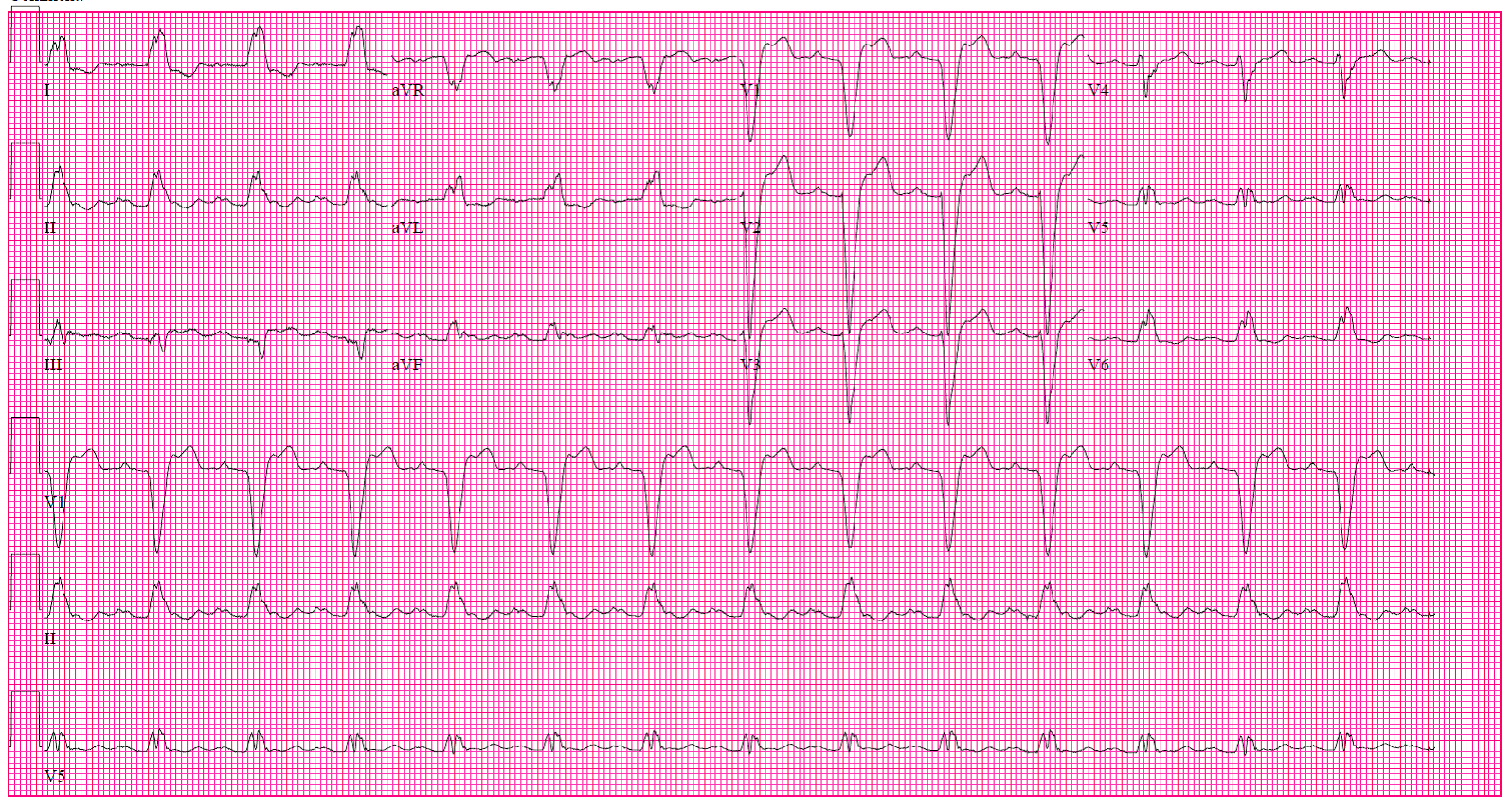
Figure 1:
The ECG shows which of the following?
Show Answer
The correct answer is: C. Left bundle branch block (LBBB) with 2:1 AV block.
The patient has a ventricular rate of 84 beat per minute (bpm) and an atrial rate of 166 bpm. In the presence of LBBB, the second P wave can be noted most readily as deflections immediately following the QRS particularly in leads II and V1.
Sinus tachycardia with 1:1 AV conduction is not present, given the presence of two P waves. Of note, the atrial rhythm may not be sinus in origin. The history of a prior atrial fibrillation ablation may create the substrate for a non-isthmus dependent (atypical) atrial flutter circuit. However, 2:1 sinus tachycardia, or ectopic (peri-nodal) atrial tachycardia may be present.
The ST-T changes are not primary due to ischemia, but rather secondary, due to the LBBB.
References
Ricard P, Imianitoff M, Yaïci K, et al. Atypical atrial flutters. Europace 2002;4;229–39.