42 year-old African-American female from Sudan with history of systemic lupus erythematous (SLE) of 9 years, diffuse interstitial lung disease of 3 years, and Sjogren's syndrome who presented to cardiology clinic for evaluation of pericardial effusion. 10 days prior to presentation, she developed chest pain and shortness of breath treated by her primary care physician (PCP) as "lung infection" with clarithromycin. The chest pain was described as substernal, mild (5 out of 10), intermittent, crushing, which worsened with deep inspiration or lying flat and radiated to the left shoulder. Her dyspnea worsened with minimal exertion, lying down, and she required 2-3 pillows to sleep. Due to the persistence of symptoms, her PCP ordered a chest computed tomography (CT) with contrast which revealed a large circumferential pericardial effusion (23 mm). Her medication regimen at this time included hydroxychloroquine 200mg oral twice daily, mycophenolate mofetil (MMF) 1000mg oral twice daily, low dose aspirin, trimethoprim/sulfamethoxazole 80 mg-400 mg oral daily, budesonide, and formoterol. Of note, she did not tolerate azathioprine in the past due to nausea and vomiting. Her family history was negative for autoimmune disease and denied any history of smoking or chemical exposure.
Upon presentation, her blood pressure was 100/64 mmHg, respiratory rate of 16 per minute, pulse of 84 beats per minute, temperature 36.6C and BMI of 34.3 kg/m2. Cardiovascular examination was notable for normal S1 and S2, no murmur or rubs, jugular venous pressure of 12 cm H20 with inspiratory collapse and, no pedal edema. Lungs auscultation revealed diffuse bilateral rales. Her abdomen was soft, non-tender, with normal bowel sounds. Complete blood count showed hemoglobin of 10.8 g/dl (normal: 11.5-15.5g/dL) with normal white blood count and platelets. Comprehensive metabolic panel, troponin T, and creatine kinase levels were within normal limits. C-reactive protein (CRP) level was 5.5 mg/dl (normal: 0.0-1 mg/dL), Westergren sedimentation rate (WSR) was 76 mm/hr (normal: 0-20 mm/hr) and anti-DNA assay was 660 IU/mL (normal: <30 IU/mL). Electrocardiogram showed normal sinus rhythm at 84 beats per minute without PR depression or ST elevation. Her echocardiogram showed a left ventricular ejection fraction of 64%, a moderate, circumferential pericardial effusion, septal bounce, and dilation of inferior vena cava at 20 mm with minimal collapse during inspiration (Figure 1; Video 1).
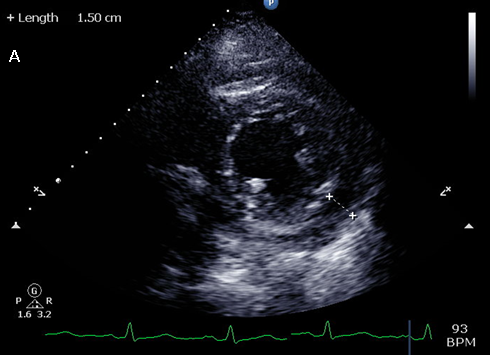
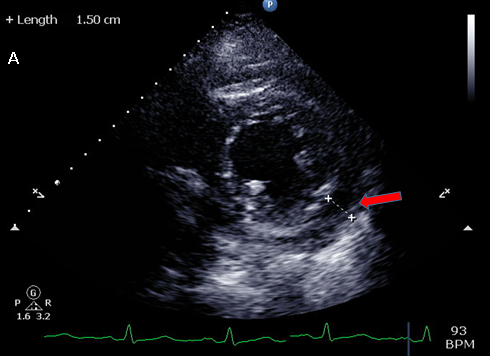
Figure 1: Transthoracic echocardiogram: parasternal short axis view (prior to pericardial window)
Video 1: Apical four chamber view on transthoracic echocardiography
Given the persistence of symptoms, significant pericardial effusion size, and for diagnostic purposes, she was referred for elective pericardial window and biopsy. 600 ml of bloody fluid was drained with improvement in her symptoms and the biopsy results revealed moderate fibrosis and chronic inflammation without any evidence of malignancy. Additional studies were remarkable for negative coxsackie antibody titers, tuberculin skin test was non-specific, likely as she received Bacillus Calmette-Guerin in the past, and her lyme antibody screen was negative.
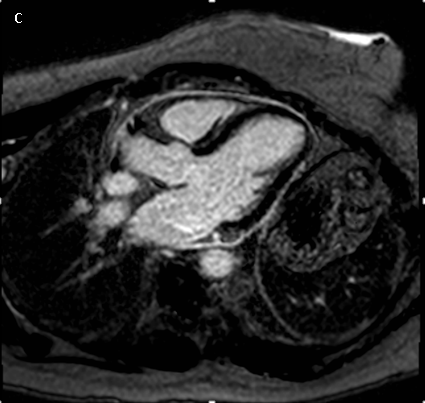
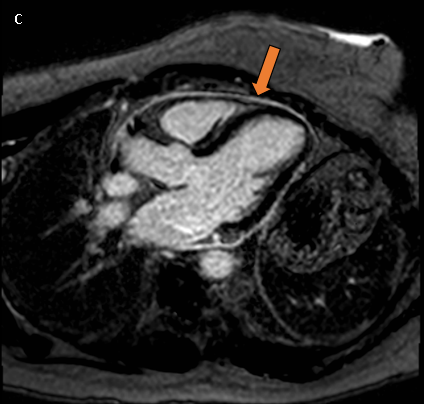
Following the pericardial window, her dyspnea and exercise capacity have improved but she is still experiencing chest pain. She underwent a cardiac magnetic resonance imaging (MRI) which showed evidence of abnormal diffuse delayed gadolinium enhancement of the visceral and parietal pericardium consistent with moderate pericardial inflammation (Figure 2 & 3; Video 2). CRP level is 2.6 mg/dl and WSR level is 53 mm/hr.
Video 2: Four chamber view on cardiac magnetic resonance imaging
Which of the following is the next best step in management?
Show Answer
The correct answer is: B. Triple therapy - ibuprofen, colchicine and 0.2-0.5 mg/kg/day prednisone.
Acute pericarditis presents as a frequent manifestation of pericardial involvement in SLE patients. Pericarditis is an indicator of active serositis which warrants a specialist opinion for a focused management approach and appropriate adjustment of medical therapy. Our patient has evidence of moderate inflammation based on elevated laboratory marker (CRP, WSR) and pericardial delayed enhancement on cardiac MRI. Her condition would be best managed with ibuprofen, colchicine and low dose prednisone. Also, in the setting of ongoing inflammation it is recommended to closely follow the patient for any evidence of recurrence. Most importantly, management of these patients requires concomitant adequate control of underlying autoimmune disease activity. Aggressive treatment with immunosuppressive agents like MMF is usually followed by a maintenance regimen to prevent flares. MMF is a steroid sparing agent which suppresses antibody production by inhibiting proliferation of both B and T lymphocytes. In a recent observational cohort study on 177 SLE patients, it revealed MMF was an effective agent in refractory lupus conditions with improved disease control.1 There is also emerging evidence that MMF might be better tolerated long term compared to azathioprine in patients with SLE as in our patient.2
Currently there are no American Heart Association/American College of Cardiology pericardial guidelines, but the 2015 European Society of Cardiology (ESC) guidelines on diagnosis and management of pericardial diseases recommends treating the predisposing systemic autoimmune disorder in patient with pericarditis. Treatment of pericarditis usually includes non-steroidal anti-inflammatory agents (NSAIDS) and colchicine; followed by addition of corticosteroid if required. The combination of the three (ibuprofen, colchicine and prednisone), "triple therapy," might be warranted in certain cases especially with continued symptoms and frequent relapses. However, the role of prednisone can become limited because of its propensity to cause more recurrences (especially in viral-induced etiologies), corticosteroid dependence, and other established adverse effects. Anakinra, intravenous immunoglobulin (IVIG), or azathioprine could be considered as subsequent therapy options if symptoms persists despite optimal triple therapy. Pericardiectomy could also be explored as an alternative but as a last possible resort after extensive discussion between the patient and the treatment team.3
Per the 2015 ESC pericardial disease guidelines, anakinra, IVIG, and azathioprine can be considered for use in patients with corticosteroid-dependent recurrent pericarditis who are not responding to colchicine (class IIb-c).3 Anakinra is an interleukin-1 receptor antagonist which has a rapid onset, is effective, and is well-tolerated. 3-year follow up studies of recurrent pericarditis patients have revealed improvement in symptoms, normalized CRP levels, discontinuation of corticosteroids use in all patients who received anakinra after a mean of 62 days, and a 95% reduction in flares.4,5 Reported side effects include local skin site inflammation, transient transaminitis, and increased risk of severe infection (especially herpes zoster).6,7 IVIGs is human serum containing diverse antibodies pooled and concentrated from thousands of healthy donors. It is widely used for autoimmune diseases because of its anti-inflammatory and immunomodulatory effects. Based on review of published studies, IVIG is helpful during acute attacks of pericarditis and considered a clinically efficacious steroid sparing agent. However, major limitations are high cost, safety concerns of infusing human plasma, requiring hospitalization for administration, and risk of recurrence upon discontinuation.8,9 Given the patient's condition, anakinra or IVIG are not indicated as the next line of treatment unless the current regimen is failing. Azathioprine is a slow-acting steroid sparing agent which is a derivative of mercaptopurine that halts DNA replication by incorporating itself into replicating DNA. It should be used cautiously under expert consultation due to risk of serious infections, hepatotoxicity, myelosuppression including increased risk for development of malignancies (especially lymphoma and skin cancer).9-11 The patient was previously intolerant of this medication due to nausea and fatigue, thus we would not recommend re-initiation of this agent.
Considering the patient's symptoms, she was recommended to start ibuprofen, colchicine and prednisone with close follow-up in clinic. At her subsequent appointments, she will be assessed for the degree of inflammation based on her symptom burden, inflammatory markers, and a repeat cardiac MRI to determine if it would be appropriate to initiate tapering of her prednisone at rate of 5 mg every 2 weeks.
Figure 1: Echocardiogram: parasternal short axis view showing a moderate circumferential pericardial effusion (red arrow).
Figure 2: Cardiac MRI delayed gadolinium-enhancement analysis (inversion recovery gradient echo sequence) after injection of gadolinium-chelate short axis view showing delayed hyperenhancement (orange arrow) consistent with moderate pericardial inflammation.
Figure 3: Cardiac MRI delayed gadolinium-enhancement analysis (inversion recovery gradient echo sequence) after injection of gadolinium-chelate three chamber view showing delayed hyperenhancement (orange arrow) consistent with moderate pericardial inflammation.
Video 1: Transthoracic echocardiogram: Apical four chamber view showing a diastolic septal bounce.
Video 2: Cardiac MRI four chamber view showing a diastolic septal bounce.
References
Tselios K, Gladman DD, Su J, Urowitz MB. Mycophenolate mofetil in nonrenal manifestations of systemic lupus erythematosus: an observational cohort study. J Rheumatol 2016;43:552-8.
Feng L, Deng J, Huo DM, Wu QY, Liao YH. Mycophenolate mofetil versus azathioprine as maintenance therapy for lupus nephritis: a meta-analysis. Nephrology 2013;18:104-10.
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;26:2921-64.
Lazaros G, Imazio M, Brucato A, et al. Anakinra: an emerging option for refractory idiopathic recurrent pericarditis: a systematic review of published evidence. J Cardiovasc Med 2016;17:256-62.
Finetti M, Insalaco A, Cantarini L, et al. Long-term efficacy of interleukin-1 receptor antagonist (anakinra) in corticosteroid-dependent and colchicine-resistant recurrent pericarditis. J Pediatr 2014;164:1425-31.
Rossi-Semerano L, Fautrel B, Wendling D, et al. Tolerance and efficacy of off-label anti-interleukin-1 treatments in France: a nationwide survey. Orphanet J Rare Dis 2015;10:19.
Brucato A , Imazio M, Gattorno M, et al. Effect of anakinra on recurrent pericarditis among patients with colchicine resistance and corticosteroid dependence: the AIRTRIP randomized clinical trial. JAMA 2016;316:1906-12.
Gelfand E. Intravenous immune globulin in autoimmune and inflammatory diseases. N Engl J Med 2012;367:2015-25.
Imazio M, Lazaros G, Brucato A, Gaita F. Recurrent pericarditis: new and emerging therapeutic options. Nat Rev Cardiol 2016;13:99-105.
Imazio M, Adler Y, Charron P. Recurrent pericarditis: modern approach in 2016. Curr Cardiol Rep 2016;18:50.
Aronson JK. Azathioprine and mercaptopurine. Meyler's side effects of drugs. Waltham, Massachusetts: Elsevier 16th Ed. 2016: 759-81.