Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
A 41-year-old man presents to the emergency department with left hand and upper extremity weakness and numbness, as well as left lower facial numbness.
Past surgical history is notable for surgical valvotomy on day of life four (1974) for pulmonary valve stenosis. He did well thereafter, and at three-year follow-up, his family was told that he was healthy and no longer needed ongoing cardiac care. His primary care physician follows him for hyperlipidemia, for which he is on a daily aspirin and statin medication. He is a never smoker and has no significant family history of coronary or cerebrovascular disease.
During his admission, his neurologic symptoms nearly resolve with the exception of left thumb numbness. He is diagnosed with a cerebrovascular accident and his evaluation included head computed tomography (normal), carotid duplex ultrasound (normal), hypercoaguable evaluation (normal), and echocardiogram to evaluate for patent foramen ovale.
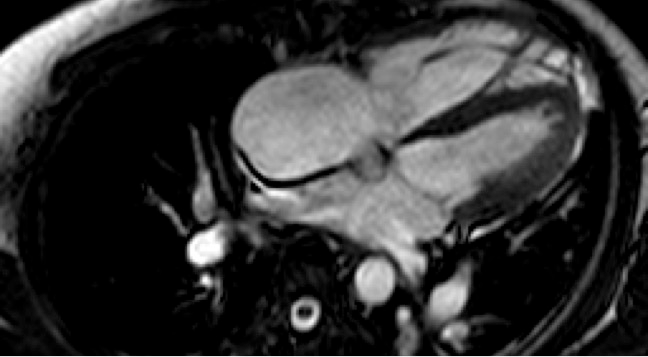
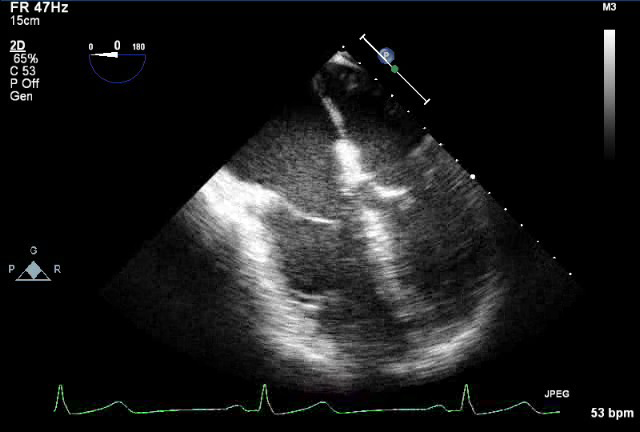
The echocardiogram demonstrates a small left-to-right atrial level shunt, dilated right ventricle, severe pulmonary valve insufficiency, and moderate tricuspid insufficiency. Exercise stress test reveals mild, non-specific ST-T changes with maximal workload of 13.7 METS.
Figure 1
Figure 2
Video 1
Which of the following statements describes the next step in the management of this patient?
Show Answer
The correct answer is: D. Cardiac magnetic resonance imaging (MRI) and electrocardiogram (ECG) and Holter monitoring.
Quantification of right ventricular (RV) size and function cannot be accurately assessed by echocardiography. Cardiac MRI is now considered the gold standard for RV evaluation.1,2 The RV end-diastolic and systolic volumes can be accurately measured as well as the RV ejection fraction and pulmonary valve regurgitant volume and fraction. RV volumes indexed to body surface area have become the accepted criteria used to determine operative timing, though the threshold varies by institution. In addition, decreased RV function, particularly in patients followed with serial MRI imaging, is considered an indication for intervention. ECG (QRS duration >180 ms) and Holter monitoring can reveal pathologic arrhythmias (ventricular tachycardia, atrial fibrillation and IART/flutter) that in and of themselves are an indication to intervene.3,4
The patient has suffered a stroke attributed to paradoxical emboli, which is an indication for closure of the atrial septal level shunt, thus medical management alone is not appropriate.
First, one would need to obtain imaging data (MRI) to evaluate if this patient meets criteria for pulmonary valve replacement in the setting of severe pulmonary insufficiency prior to referral to Interventional Cardiology. The patient would not be a candidate for transcatheter pulmonary valve replacement without a landing zone for the percutaneous valve.
Cardiac catheterization is usually not necessary unless the coronary anatomy needs to be determined, such as in patients with tetralogy of Fallot where the original operative note does not clearly describe the anatomy, or when coronary artery disease needs to be evaluated. This patient performed well on his stress test and preoperative cardiac catheterization showed normal coronaries without evidence of coronary artery disease.
Operative correction is most likely indicated, but further imaging is warranted as next step.
ECG: NSR, left atrial enlargement, QRS duration 96 ms
Holter: Predominant rhythm is sinus. Occasional multiform premature ventricular complexes (~22/hour). No ventricular tachycardia. Rare isolated premature atrial complexes (~1/hour). No symptoms recorded.
Based on the patient's RV dilation, he was indicated for pulmonary valve replacement in addition to closure of the atrial septal level shunt. The pulmonary valve was replaced with a 29 mm porcine prosthesis. Intracardiac examination of the atrial septum identified a stretched patent foramen ovale, which was closed primarily. The tricuspid annulus was found to be dilated, and in the setting of moderate-to-severe regurgitation on preoperative transesophageal echocardiogram, a tricuspid valuloplasty (34 mm annuloplasty band) was performed. Postoperative demonstrated no pulmonary valve insufficiency, bilateral pulmonary venous return, normal RV function, trivial tricuspid insufficiency and no residual atrial level shunt. He had an uneventful recovery. After surgical follow-up is complete, he is scheduled for routine follow-up with a cardiologist with expertise with adult congenital heart disease in addition to his primary care physician.5
Discussion
The prevalence of pulmonary stenosis is 8-12% of all congenital heart defects. Isolated pulmonic valvular stenosis with intact ventricular septum is the second most common congenital cardiac defect, with bicuspid aortic valve being the most common. Pulmonic valvular stenosis may occur in as many as 30% of all patients who have other congenital heart defects.
There is limited information regarding the long-term follow-up of patients with surgically corrected pulmonary stenosis; however, it is known that ~80% will require some sort of intervention by their fifth decade of life and thus must be followed. The American College of Cardiology (ACC)/American Heart Association (AHA) guidelines recommend follow-up with a cardiologist with expertise in adult congenital heart disease no less frequently than every five years (annually for patients with tetralogy of Fallot).6
One study reviewed the long-term outcome of 53 patients after surgical valvotomy performed for pulmonary stenosis between 1951 and 1982. At median follow-up of 34 years, 53% of patients had undergone reintervention with the majority (75%) being pulmonary valve replacement with other interventions for atrial septal defect, residual pulmonary stenosis, right ventricular outflow tract obstruction, closure of iatrogenic ventricular septal defect, ligation of aortopulmonary fistula and tricuspid valvuloplasty with simultaneous coronary bypass grafting. Atrial and ventricular arrhythmias were common, occurring in 38% of patients.7
The ACC/AHA guideline indications for pulmonary valve replacement after surgical valvotomy for pulmonary stenosis are RV enlargement prior to becoming severe, any RV dysfunction worse than mild, deteriorating exercise capacity or the onset of atrial or ventricular arrhythmias.7
Isolated pulmonary stenosis patients who underwent neonatal intervention share some of the same long-term complications that result after surgical repair of tetralogy of Fallot, vis-à-vis free pulmonary insufficiency and its implications for the right heart. Tetralogy of Fallot represents the largest adult congenital population currently, owing to the fact that this was one of the first lesions surgically repaired.
The late survival for TOF after repair is excellent with 35 year survival of approximately 85% and likely better for isolated pulmonary stenosis patients. Despite this, there is a concerning incidence of unexpected sudden cardiac death during long-term follow-up of tetralogy of Fallot patients and though not an identical population and it may be prudent to consider this data when evaluating a patient with repaired pulmonary stenosis. Ventricular tachycardia is the mechanism responsible for most of these deaths, though intra-atrial reentrant tachycardia (IART/flutter) and AV block may be responsible in some cases. Pulmonary stenosis patients have not undergone ventricular septal defect repair and, thus, are less likely to have right fascicular block as is common in tetralogy of Fallot patients but, as described above, do commonly suffer from ventricular and atrial arrhythmias. The incidence of sudden cardiac death in repaired TOF is 2.5% per decade of follow-up.8,9
References
Davlouros PA, Kilner PJ, Hornung TS, et al. Right ventricular function in adults with repaired tetralogy of Fallot assessed with cardiovascular magnetic resonance imaging: detrimental role of right ventricular outflow aneurysms or akinesia and adverse right to left ventricular interaction. J Am Coll Cardiol 2002;40:2044-52.
van Straten A, Vliegen HW, Hazekamp MG, de Roos A. Right ventricular function late after total repair of tetralogy of Fallot. Eur Radiol 2005;15:702-7.
Harrison DA, Harris L, Siu SC, et al. Sustained ventricular tachycardia in adult patients late after repair of tetralogy of Fallot. J Am Coll Cardiol 1997;30:1368-73.
Harrison DA, Siu SC, Hussain F, MacLoghlin CJ, Webb GD, Harris L. Sustained atrial arrhythmias in adults later after repair of tetralogy of Fallot. Am J Cardiol 2001;87:584-8.
Landzberg MJ, Murphy DJ Jr, Davidson WR Jr, et al. Task Force 4: organization of delivery systems for adults with congenital heart disease. J Am Coll Cardiol 2001;37:1187-93.
Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults With congenital heart disease. J Am Coll Cardiol 2008;52:e143-263.
Earing MR, Connolly HM, Dearani JA, Ammash NM, Grogan M, Warnes CA. Long-term follow-up of patients after surgical treatment for isolated pulmonary valve stenosis. Mayo Clin Proc 2005;80:871-6.
Nollert G, F. T. Long-term survival in patients with repair of tetralogy of Fallot: 36-Year follow-up of 490 survivors of the first year afer surgical repair. J Am Coll Cardiol 1997;30:1374-83.
Gatzoulis MA, Balaji S, Webber SA. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet 2000;356:975-81.