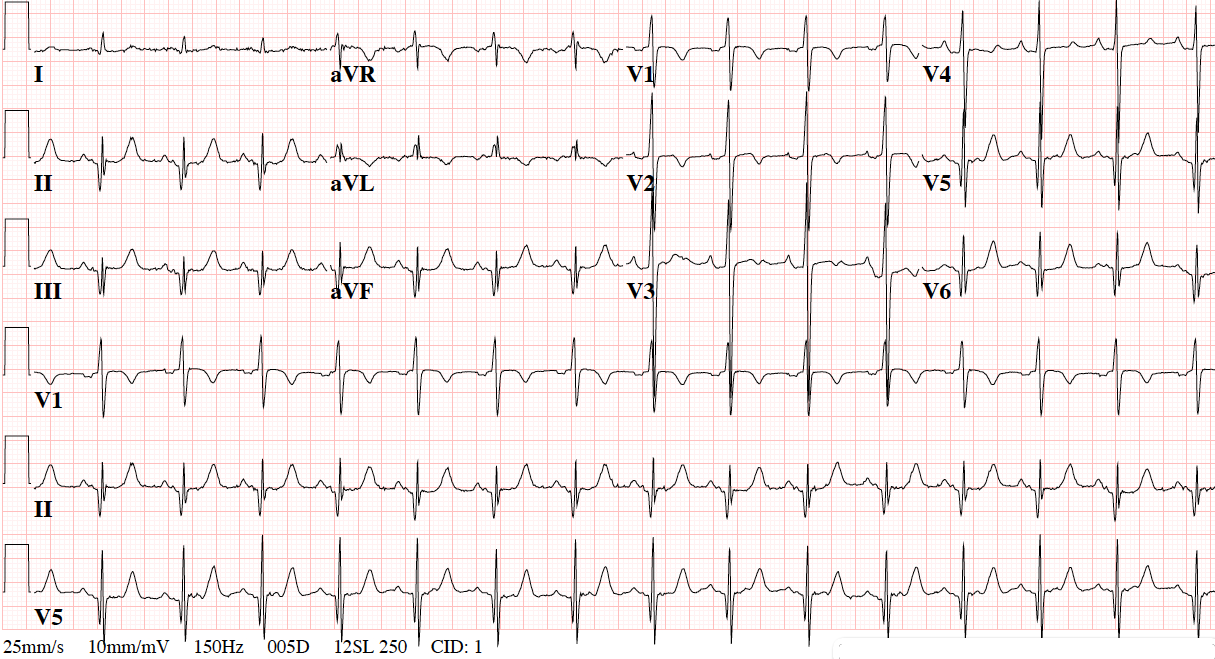
A 71-year-old woman with no history of cardiovascular disease is evaluated for elective thoracotomy with wedge resection of a left lower lobe lung mass. She is an active smoker with a chronic cough, but denies cardiac symptoms. She has no history of hypertension, diabetes, heart failure, or renal disease. A "routine" preoperative electrocardiogram (ECG) is obtained as shown (Figure 1), and she is referred for cardiology consultation to address the result.
Figure 1
You are asked to review the electronic health record and recommend next steps. The anesthesiology service notes that her Duke Activity Score Index estimates 9 METS of daily activity. You choose to do which of the following?
Show Answer
The correct answer is: B. Obtain a resting transthoracic echocardiogram.
The patient may undergo high-risk surgery, and further investigation is warranted. ECGs with hypertrophic cardiomyopathy (HCM) (asymmetric septal hypertrophy) may be variable and pleomorphic across individuals-remarkable, they may change with time in same subject. Salient ECG features range from grossly normal appearing to pseudoinfarct patterns. Specifically, the presence of prominent (but typically narrow) Q waves in the inferolateral leads may be concerning for a recent or prior myocardial infarction (MI). However, these reflect initial septal depolarization, and may be seen in left ventricular septal hypertrophy, essential hypertension, or hypertrophic cardiomyopathy. Also often seen, and manifested in this case, is a tall R in lead V1/V2 due to septal hypertrophy, with slow or absent R wave progression in V1-V3.
Resting echo would be the most cost-effective and accurate means to identify HCM or a large prior infero-lateral infarction.
Choice A is incorrect as intrathoracic surgery is considered high-risk, and an abnormal ECG justifies further preoperative risk stratification.
Choice C is incorrect because echocardiography is of lower cost, and more accurate for differentiating infarction from hypertrophy, particularly when due to HCM.
Choice D is incorrect because the patient is asymptomatic, and further risk stratification with non-invasive imaging should be obtained first.
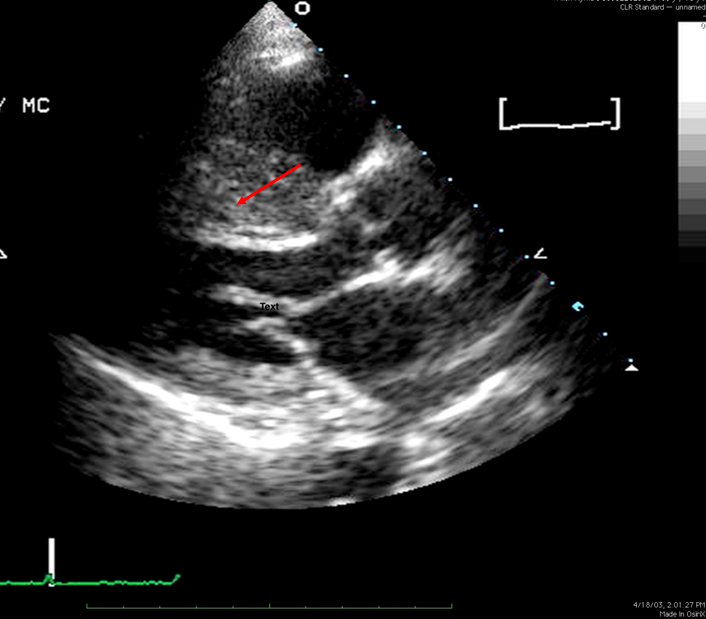
This patient was sent for Adenosine Thallium stress testing prior to cardiology consultation. A medium-sized mild defect was seen in the anterior and inferolateral walls, and she was then referred to cardiology. Transthoracic echo revealed asymmetric septal hypertrophy as shown (Figure 2), with no resting left ventricular outflow tract (LVOT) gradient or mitral regurgitation, and a late systolic 40 mm Hg LVOT gradient during Valsalva. She underwent cardiac catheterization to address the Thallium perfusion result, and had only mild luminal irregularities on coronary angiography, with normal wall motion on ventriculography, and no resting LVOT gradient. She was released to undergo wedge resection, complicated only by postoperative atrial fibrillation.
Early recognition of this possible diagnosis may have prevented the use of perfusion imaging and cardiac catheterization.
Figure 2
References
Gersh BH, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011;124:2761-96.
Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;130:2215-45.
Please share your thoughts on this Patient Case Quiz in the comments section below.
Please note: You may identify yourself via the "Guest" fields, but there is no additional need to login to ACC.org in order to comment.
NEW! Improve your ECG interpretation skills with ECG Drill & Practice
This program reviews key findings in clinical electrocardiography and also contains a self-assessment ECG test, featuring the format and answer options similar to those of the ABIM’s certifying examination in cardiovascular disease. It’s a great resource for anyone preparing for initial Board certification in CV disease and for anyone looking to hone their ECG interpretation skills.