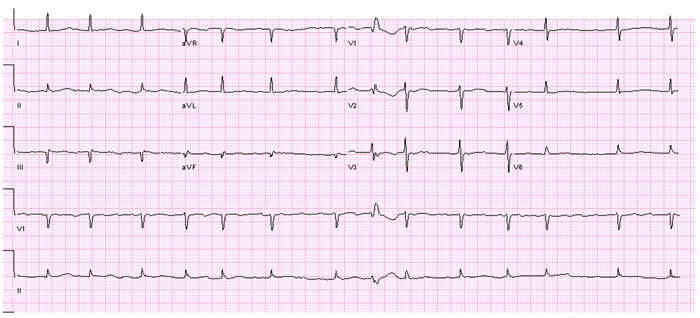
A 66-year-old gentleman with persistent atrial fibrillation (AF) for over 10 years presents to the clinic for evaluation of highly symptomatic AF causing fatigue, exertional shortness of breath and palpitations. His CHADS2VASc score is 4 and he currently takes warfarin anticoagulation. He failed sotalol in the past and has received multiple cardioversions (6 over 5 years) in attempts to maintain sinus rhythm. He underwent wide area circumferential ablation for pulmonary vein isolation, and a linear left atrial roof ablation 2 years prior to this presentation. However, he continues to have highly symptomatic break though episodes of AF on another anti arrhythmic drug dofetilide.
Pertinent past medical history also includes hypertension, transient ischemic attacks and hepatitis B, as well as prior AF ablation.
Medications:
Warfarin for target INR 2.0- 3.0, diltiazem SA 360mg once daily, dofetilide 250 mcg twice daily, losartan 100mg once daily, sildenafil 25mg once daily, Vitamin D3 2000 units daily and Calcium carbonate 500mg three times daily.
Physical Exam:
Vital signs: Heart rate 110 beats/min in AF in clinic, BP 145/92 mm hg, RR 18, Afebrile, BMI 30
General: Alert, Comfortable and oriented to time, place and person
Neck: 9 cm JVD
CV: Irregularly irregular, No murmurs noted
Lungs: Clear to auscultation
Abdomen: soft tender without any masses
Extremities: No pedal edema
Neurological exam: No gross neurological deficits
Pertinent Labs and echocardiographic parameters:
TSH: 2.69 (Range 0.49-4.69 mIU/ml)
Serum Creatinine- 1.11 (Range 0.4-1.2 mg/dl)
Echocardiogram: Normal left ventricular size, thickness and function (LVEF 60%). Left atrial enlargement (left atrial diameter 62 mm). No significant valvular abnormalities noted.
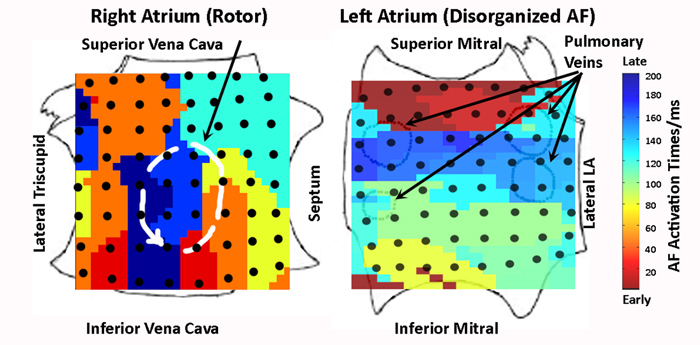
After a discussion of treatment alternatives, risks and benefits, the patient was taken to the electrophysiology laboratory for repeat ablation. Under specific IRB approved informed consent, AF was mapped prior to ablation using a new approach (Focal Impulse and Rotor Mapping, FIRM) by inserting a 64 pole basket catheter (Constellation, Boston Scientific, MA) into the right then left atria in turn. FIRM maps reveal the following maps of AF activation:
Activation during AF is color coded from early (red) to late (blue). A rotor is seen in the posteroinferior right atrium (indicated by a red-to-blue spiral wave), while the left atrium shows very disorganized activity. Key: The right atrium is opened at a meridian, with reflection of the lateral and medial tricuspid annuli. The left atrium is opened at its equator, with reflection of the superior and inferior mitral annuli. The pulmonary vein orifices (left atrium) are labeled.
Based on the above information, the step most likely to treat this man’s AF would be:
Show Answer
The correct answer is: C. Targeted ablation of AF rotor in the right atrium (Focal Impulse and Rotor Modulation, FIRM).
Symptomatic persistent atrial fibrillation (AF) refractory or intolerant to at least one class I or III antiarrhythmic drug is a class 2A indication for catheter ablation.(1) The AFFIRM trial(2) showed that either rate control or rhythm control have similar outcomes, but since our patient has significant AF symptoms he may benefit from remaining in sinus rhythm. Since he has already failed two potent anti-arrhythmic medications, AF ablation was considered an attractive option.
Ablation for AF is based on the concept that AF is initiated by triggers then continued by distinct sustaining mechanisms. Theoretically, either may be ablated. Our patient had already received pulmonary vein isolation to isolate triggers(1), yet unfortunately showed little improvement. Notably, although pulmonary vein ectopic beats may trigger AF, it is unclear what mechanisms sustain human AF after it has been triggered.
There are two prevailing hypotheses for AF-sustaining mechanisms in humans: the Multiple wavelet hypothesis(3), in which spatially disorganized waves meander within the atria, and the Localized source hypothesis, in which localized and rapidly activating reentrant circuits (rotors)(4) or focal impulses(5) drive AF. The multiple wavelet hypothesis does not fully explain observed non-uniformities in AF, or the fact that AF may terminate relatively early during ablation before atrial ‘debulking’ has been achieved. Conversely, while several animal studies demonstrate localized sources, there had until recently been only indirect evidence(6,7) for their existence in human AF.
A novel approach to computational mapping(9,10) recently demonstrated that localized rotors or focal impulses are highly prevalent in human AF, and are sites where very brief targeted ablation (Focal Impulse and Rotor Modulation, FIRM) terminated or dramatically slowed AF with substantially improved long-term AF elimination versus conventional therapy alone in the CONFIRM (CONventional ablation for atrial fibrillation with or without Focal Impulse and Rotor Modulation) trial.(9)
FIRM mapping in our patient (RhythmViewTM, Topera, San Diego, California) revealed a sustained counterclockwise rotor in the right atrium, with disorganized AF in the left atrium (Figure 2). Accordingly, we performed targeted ablation (FIRM) at only this right atrial rotor. FIRM terminated AF in 48 seconds to sinus rhythm, prior to any other ablation. AF was now very difficult to re-initiate. Minimal touch-up to the pulmonary veins was performed and the case was concluded. A continuous ECG monitor with AF autodetection algorithm was implanted (Reveal XTTM, Medtronic, Minneapolis, MN), and the patient remains symptom and arrhythmia free off anti-arrhythmic medications at 1 year.
Turning to the alternative answers, the strategy (A) of re-isolating the pulmonary veins alone is associated with suboptimal outcome in patients with persistent AF.(8) The strategy (B) of pulmonary vein isolation with additional linear lesions, potentially with isolation of the superior vena cava and ablation of complex fractionated atrial electrograms may enable up to 70-80% freedom from AF after three or more procedures(1). However, this comes at the expense of a substantial incidence of iatrogenic atrial tachycardia1 and potential side-effects including stiff left atrial syndrome(11). The option (D) of ablating the atrioventricular junction with permanent pacing is viable, but leaves the patient in AF without atrial transport function. Furthermore, the patient and physician had already decided to pursue AF ablation, and the ability to map the RA rotor motivates FIRM ablation. In the CONFIRM trial(9), FIRM guided ablation with conventional ablation eliminated AF in 84% of patients compared to 50% with conventional ablation alone at 2 years (using implanted ECG monitors in 84% of FIRM-guided patients).
Note: Use of the Constellation catheter in the left atrium is an off-label usage.
References
Calkins H, Brugada J, Packer DL, et al. HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart rhythm 2007; 4:816-861.
Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002; 347:1825-1833.
Allessie MA, de Groot NM, Houben RP, et al. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease: longitudinal dissociation. Circ Arrhyth Electrophysiol 2010; 3:606-615.
Vaquero M, Calvo D, Jalife J. Cardiac fibrillation: from ion channels to rotors in the human heart. Heart Rhythm 2008; 5:872-879.
Takahashi Y, Hocini M, O'Neill MD, et al. Sites of focal atrial activity characterized by endocardial mapping during atrial fibrillation. J Am Coll Cardiol 2006; 47:2005-2012.
Sanders P, Berenfeld O, Hocini M, et al. Spectral analysis identifies sites of high-frequency activity maintaining atrial fibrillation in humans. Circulation 2005; 112:789-797.
Atienza F, Almendral J, Moreno J, et al. Activation of inward rectifier potassium channels accelerates atrial fibrillation in humans: evidence for a reentrant mechanism. Circulation 2006; 114:2434-2442.
Cheema A, Dong J, Dalal D, et al. Circumferential ablation with pulmonary vein isolation in permanent atrial fibrillation. Am J Cardiol 2007; 99:1425-1428.
Narayan SM, Mittal S. et al. Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation: The CONFIRM Trial (Late Breaking Clinical Trial Abstract). Heart Rhythm 2011; 8:LB-04.
Narayan SM, Krummen DE, Rappel W-J. Clinical Mapping Approach To Diagnose Electrical Rotors and Focal Impulse Sources for Human Atrial Fibrillation. J Cardiovasc Electrophysiol 2012: In Review.
Gibson DN, Di Biase L, Mohanty P, et al. Stiff Left Atrial Syndrome Following Catheter Ablation for Atrial Fibrillation: Clinical Characterization, Prevalence and Predictors. Heart Rhythm 2011; 8:1364-71.