A 56-year-old man with past history of coronary artery disease (status post-stent placement to mid left anterior descending artery 5 years ago), diabetes mellitus, and hypertension presented with complaint of acute substernal chest pressure for the past half hour. He was smoking marijuana with his friends about 1 hour prior. The pain was similar to the chest pain that he experienced 5 years ago that resulted in stent placement. He is a current smoker, social drinker, and smokes marijuana occasionally. Physical examination revealed a man with moderate discomfort and with injected conjunctiva. Cardiac and lung examination were normal.
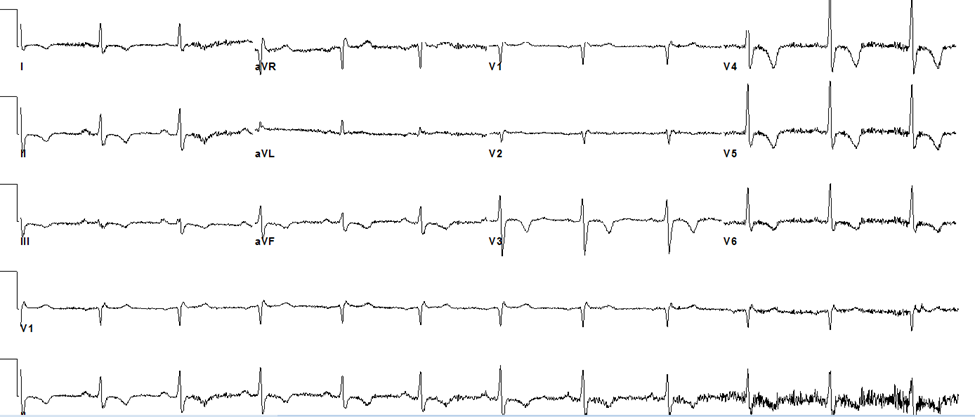
Vital signs were a heart rate of 110 bpm, blood pressure of 148/92 mmHg, and afebrile status. Initial troponin I was 0.6 ng/ml (normal is <0.05 ng/ml), which peaked to 2.10 ng/ml 6 hours later. Electrocardiography was performed (Figure 1).
Figure 1
The correct answer is: B. Marijuana use increases risk of myocardial infarction (MI) immediately after use.
The patient suffered from acute coronary syndrome—non-ST-segment elevation MI—suggested by typical chest pain, troponin elevation, and changes in the electrocardiogram that are suggestive of ischemia. Marijuana use is known to trigger MI. It increases the risk of MI by 4.8 times within 1 hour of use. Comparative risk assessment suggests that cocaine is more likely to trigger an MI than marijuana. Cocaine has an odds ratio of 24 compared with an odds ratio of 4.8 for marijuana for triggering an MI.1 Large sample size, long-term studies like the CARDIA (Coronary Artery Risk Development in Young Adults) study failed to show any association between marijuana and cardiovascular risk after adjusting for confounding factors.2 However, in patients who have survived acute MI, marijuana use more than once a week is associated with a threefold increase in mortality.3 Marijuana-induced sympathetic stimulation increases myocardial oxygen demand. This, along with a decreased oxygen supply due to carboxyhemoglobin formation from inhalation of products of combustion in marijuana cigarettes, decreases the time to angina in patients with stable coronary artery disease.4 Therefore, marijuana use can precipitate an acute event in susceptible patients, and its use may be associated with increased mortality in patients with a history of MI.
References
- Nawrot TS, Perez L, Künzli N, Munters E, Nemery B. Public health importance of triggers of myocardial infarction: a comparative risk assessment. Lancet 2011;377:732-40.
- Rodondi N, Pletcher MJ, Liu K, Hulley SB, Sidney S; Coronary Artery Risk Development in Young Adults (CARDIA) Study. Marijuana use, diet, body mass index, and cardiovascular risk factors (from the CARDIA study). Am J Cardiol 2006;98:478-84.
- Mukamal KJ, Maclure M, Muller JE, Mittleman MA. An exploratory prospective study of marijuana use and mortality following acute myocardial infarction. Am Heart J 2008;155:465-70.
- Aronow WS, Cassidy J. Effect of marihuana and placebo-marihuana smoking on angina pectoris. N Engl J Med 1974;291:65-7.