An 80-year-old male patient with rheumatic heart disease, bio-prosthetic aortic valve, stage IV non-small cell lung cancer, and brain metastases presented with progressive shortness of breath and worsening pleural effusions. He had no history of systemic embolization and was not on anticoagulation. On exam, he was hemodynamically stable at presentation with an elevated jugular venous pressure and bilateral pedal edema. Transthoracic echocardiographic imaging revealed the presence of new onset severe cardiomyopathy with an ejection fraction of 30% and global hypokinesis.
Video 1
Two-dimensional imaging of the apical four-chamber view demonstrating large biventricular thrombi with mobile components.
Video 2
Inversed apical four-chamber view on transthoracic echocardiogram with contrast to better characterize intra-ventricular thrombi. The left ventricle is shown on the left side in the clip.
What is your diagnosis based on the imaging?
Show Answer
The correct answer is: C. Biventricular thrombi
These findings are consistent with the diagnosis of massive biventricular thrombosis in a patient with severe cardiomyopathy from unknown etiology that is complicated by an underlying hypercoagulable state secondary to malignancy leading to the formation of clot. There was no evidence of pericardial and myocardial involvement or of metastasis of primary tumor into the ventricular cavity.
Two-dimensional echocardiographic imaging with and without contrast show the presence of large biventricular masses with mobile components occupying at least 50% of ventricular cavities that were characterized as thrombi (Videos 1-2). Retrospective inspection of a recently performed non-gated computed tomography of the chest revealed findings consistent with the presence of biventricular thrombosis in the absence of evidence for myocardial involvement or infiltration (Figure 1). Following admission, the patient's hospital course deteriorated quickly, unfortunately complicated by shock, and resulted in disseminated intravascular coagulation and eventually death.
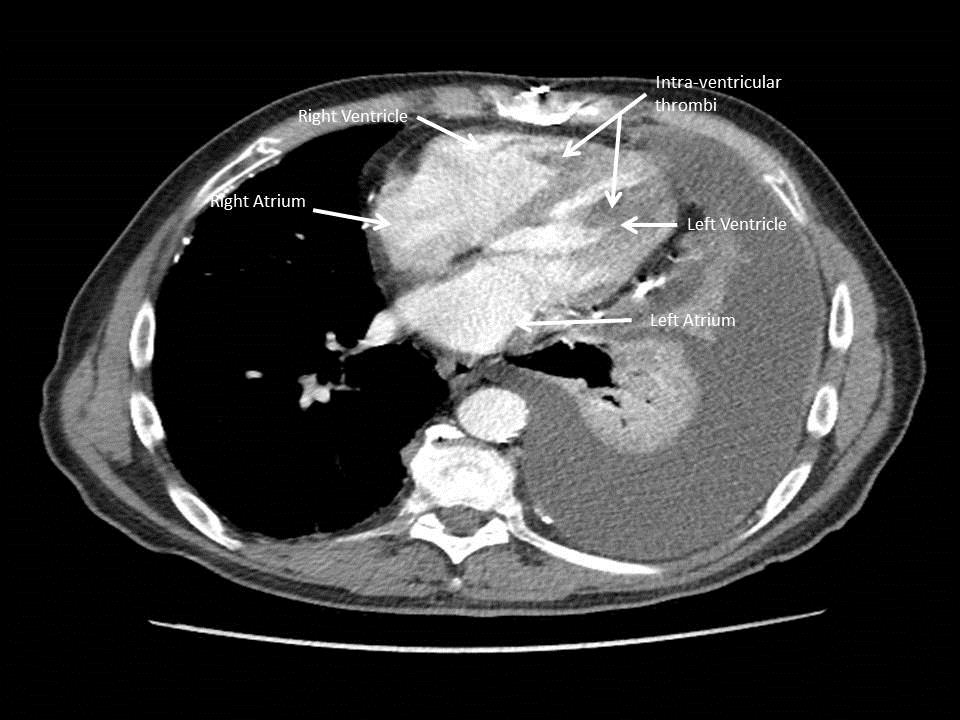
Figure 1
Computed tomography of the chest with contrast showing the presence of intra-ventricular densities in both ventricles suggestive of clot.
Ventricular thrombus is a potentially life-threatening condition and puts patients at an increased risk for embolic complications, including stroke or pulmonary embolism depending on the site. Cases of biventricular thrombi are reported in literature in patients with severe biventricular dysfunction, commonly in the setting of hypercoagulable mileu such as pregnancy, HIV-associated dilated cardiomyopathy, malignancy, and myocardial infarction. The clinical course involves full-dose anticoagulation with serial repeat imaging, and the prognosis may depend on underlying etiology and reversibility of ventricular dysfunction. Surgical removal of the clot may be considered in select cases. Characteristics such as subacute thrombosis and large mobile clots extending all the way into the ventricular outflow tract are more likely to embolize.
Primary cardiac tumors are extremely rare, with an incidence of less 0.02% according to one autopsy series. Myxoma is the most common primary cardiac tumor and is typically benign, pedunculated with gelatinous consistency, has smooth and lobulated surfaces, and originates predominantly in the left atrium followed by the right atrium. Metastatic involvement of the heart is more common than primary cardiac involvement and is mostly seen with disseminated tumor disease. Tumors that are most likely to metastasize to the heart include melanomas, breast cancer, lung cancer, lymphomas, thyroid cancer, renal carcinoma, and esophageal cancer.
Non-compaction cardiomyopathy is a genetic cardiomyopathy characterized by excessively prominent trabeculation of the ventricles. Diagnosis is performed mainly using echocardiogram and several echocardiographic criteria such as Jenni or Chin criteria to assist in diagnosis.
References
Kim DY, Islam S, Mondal NT, Mussell F, Rauchholz M. Biventricular thrombi associated with peripartum cardiomyopathy. J Health Popul Nutr 2011;29:178-80.
Haine SE, De Ridder SM, Van de Vijver KK. Images in cardiology. Ventricular thrombi with pulmonary and systemic embolization. Can J Cardiol 2008;24:e92.
Jariwala P. Biventricular Mural Thrombi in Patients With Dilated Cardiomyopathies: Case Reports and Review. Archives of Cardiovascular Imaging 2014;2:e19863.
Missault L, Koch A, Colardyn F, Clement D. Biventricular thrombi in dilated cardiomyopathy: massive simultaneous pulmonary and systemic embolisation. Eur Heart J 1994;15:713-4.