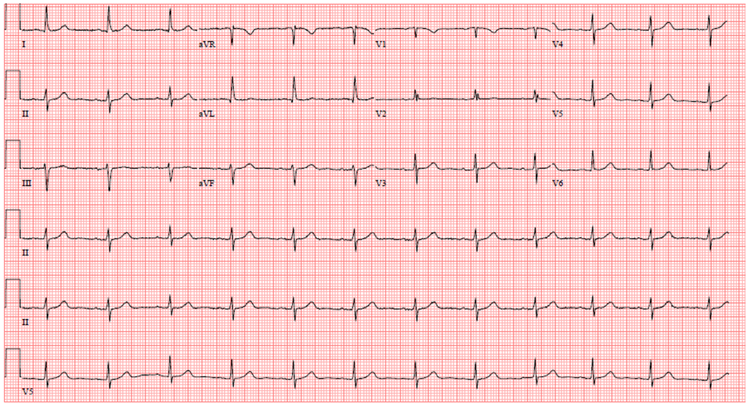
A 60-year-old man is referred to your cardiology clinic for an evaluation of chest pain. He has not seen a physician for several years prior to being evaluated by his new primary care doctor one week ago. During that visit, he mentioned episodes of sharp, left-sided chest pain that are fleeting in nature that he notices more with exertion. He does not recall any episodes of rest pain. He has a history of myocardial infarction at the age of 50 treated with stents and has not experienced any angina since then. The chest pain he describes is different from the pain he experienced with his MI. He is a former smoker and quit at the time of his MI. His only medication is aspirin, 81mg daily. He was noted to be hypertensive with a blood pressure of 152/90 mmHg with an otherwise normal physical exam. His PCP ordered an ECG (shown below) and checked labs including troponin prior to referring him. His TnT was <0.01 ng/mL. Lipid panel showed total cholesterol of 190 mg/dL, LDL 120 mg/dL, HDL 40 mg/dL.
Figure 1
Which of the following is the next best step in the management of this patient?
Show Answer
The correct answer is: 3. Initiate evidence based medical therapy including beta blocker, statin, ace-inhibitor, and prn nitroglycerin. Reassess symptoms in 4 weeks.
Explanation
The case describes a patient with stable ischemic heart disease presenting with chest pain not consistent with typical angina. His only pharmacologic therapy is aspirin. Given his symptoms and history, the best initial management includes initiation of guidelines recommended therapy to include beta-blocker, ace-inhibitor, statin, and nitroglycerin prn.1 As he is low risk, it would not be appropriate to pursue coronary angiography as the next step without high-risk features or noninvasive testing demonstrating ischemia. It would be reasonable to pursue exercise testing at this point with or without imaging, or should he develop worsening symptoms or ongoing symptoms after initiation of medical therapy. As there is no information precluding exercise and the ECG is interpretable, a pharmacologic noninvasive study would not be recommended. Although recent evidence suggests that high-sensitivity troponin may provide additional prognostic information in this setting, there is insufficient evidence to recommend routine testing, mainly as there are no additional therapies that are known to improve outcomes based on detectable levels of high-sensitivity troponin in patients with stable coronary disease.
References
Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease. J Am Coll Cardiol 2012;60:e44-e164.