|
Figure 1 (A-D)
|
|
|
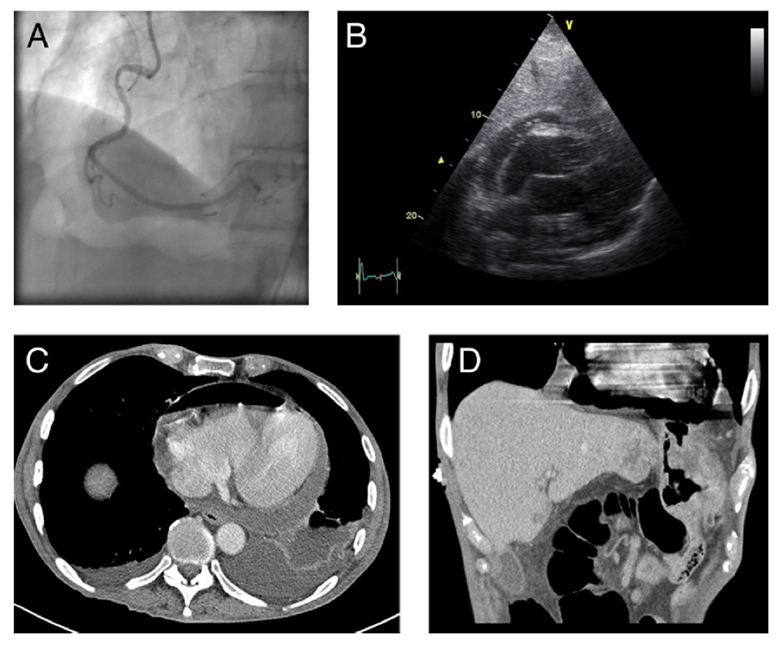
A 70-year-old man presented with sudden onset pleuritic chest pain and inferolateral ST-segment elevation on electrocardiogram via a primary percutaneous coronary intervention service. He had gastric cancer, palliated with radiotherapy. Coronary angiogram showed unobstructed arteries and a radiolucent pericardial space with a craggy surface (
A). On echocardiography there were only sub-costal windows, which showed a pericardial effusion containing mobile echo-bright densities, no tamponade, and thickening around the right atrium consistent with malignant infiltration (
B). Contrast-enhanced computed tomography (CT) showed hydropneumopericardium (
C) and a fistulous tract between the gastric fundus and pericardial space (
D).
The correct answer is: C. Acute pneumopericardium
The opening of the fistula between the stomach and pericardial space likely allowed air to suddenly rise into the pericardial space causing the acute onset of chest pain and ECG changes consistent with pericarditis. Radiation therapy in the oncological patient is a predisposing factor for such fistula formation.(1) The patient was treated palliatively and died the next day.
There were poor echo windows due to air in the pericardial space. The mobile echo-bright densities seen in the sub-costal views were air bubbles. This case highlights the value of CT in the investigation of pericardial disease.
References
- Luthi F, Groebli Y, Newton A, Kaeser P. Cardiac and pericardial fistulae associated with esophageal or gastric neoplasms: a literature review. Int Surg 2003;88:188-193.