A 46-year-old woman presented with acute substernal chest pain. The pain occurred at rest and lasted 20 minutes. It was relieved when emergency medical service gave her sublingual nitroglycerin. The physical examination revealed an anxious woman who was afebrile and normotensive. She had a normal cardiac and lung examination. The first electrocardiogram (ECG) demonstrated normal sinus rhythm with ST-T wave changes in the anterolateral and inferior leads consistent with ischemia. The first troponin I returned positive at 0.41 ng/mL. The patient was started on dual antiplatelet therapy, anticoagulation, high-dose statin therapy, and a beta-blocker.
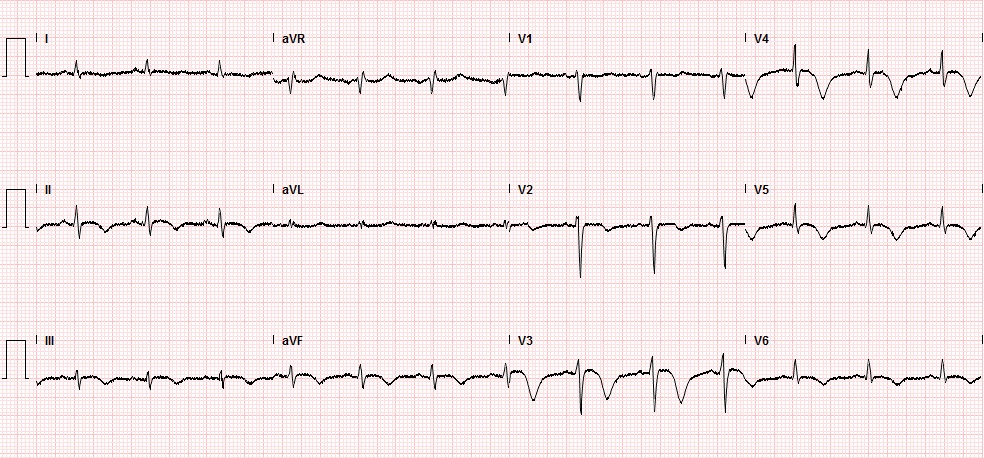
The patient remained asymptomatic overnight; however, she developed recurrent chest pain the next morning. The second troponin I returned 6.7 ng/mL, and a repeat ECG during the chest pain episode was performed (Figure 1). The patient was then taken for urgent cardiac catheterization (Figure 2).
Figure 1
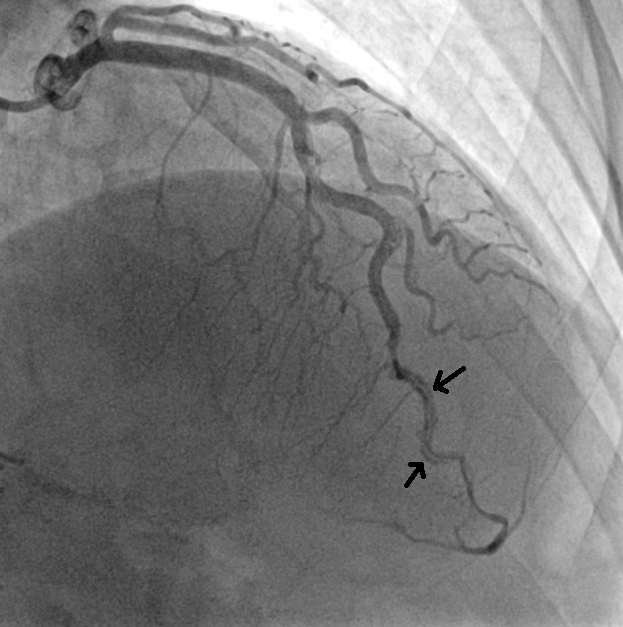
Figure 2
With regard to the diagnosis, which statement is correct?
Show Answer
The correct answer is: B. People who present with this disease usually do not have the classic risk factors for coronary artery disease.
The patient has suffered from a spontaneous coronary artery dissection. Cardiac catheterization revealed an angiographically normal left anterior descending artery until the mid-portion, where there was evidence of a dissection and caliber change from the mid-portion down to just before the apex (Figure 2). Spontaneous coronary artery dissection is an uncommon cause of ACS. However; this disease entity seems to be more common in young women, accounting for 24% of ACS in women less than 50 years old.1 People who present with spontaneous coronary artery dissection generally do not have the classic risk factors for coronary artery disease.2 In many cases, a predisposing arterial disease like fibromuscular dysplasia can be identified, but up to 20% of cases are idiopathic.2,3 The pathophysiology involves dissection and hematoma formation in the vessel media, causing luminal narrowing and obstruction.4
The diagnosis of spontaneous coronary artery dissection is made by angiography, and the optimal management is not clear. Revascularization with either PCI or coronary artery bypass grafting have been reported.1,2 A recent retrospective study of 189 patients with spontaneous coronary artery dissection demonstrated that an invasive strategy is no better in terms of outcomes (eventual target vessel revascularization and recurrent spontaneous coronary artery dissection) when compared with a conservative strategy.4 In fact, PCI for spontaneous coronary artery dissection has high rates of complications and emergency coronary artery bypass grafting, even in those presenting with preserved vessel flow.4
References
Saw J, Aymong E, Mancini GB, Sedlak T, Starovoytov A, Ricci D. Nonatherosclerotic coronary artery disease in young women. Can J Cardiol. 2014;30:814-9.
Saw J, Aymong E, Sedlak T, et al. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv. 2014;7:645-55.
Saw J, Ricci D, Starovoytov A, Fox R, Buller CE. Spontaneous coronary artery dissection: prevalence of predisposing conditions including fibromuscular dysplasia in a tertiary center cohort. JACC Cardiovasc Interv 2013;6:44-52.
Tweet MS, Eleid MF, Best PJ, et al. Spontaneous coronary artery dissection: revascularization versus conservative therapy. Circ Cardiovasc Interv 2014;7:777-86.