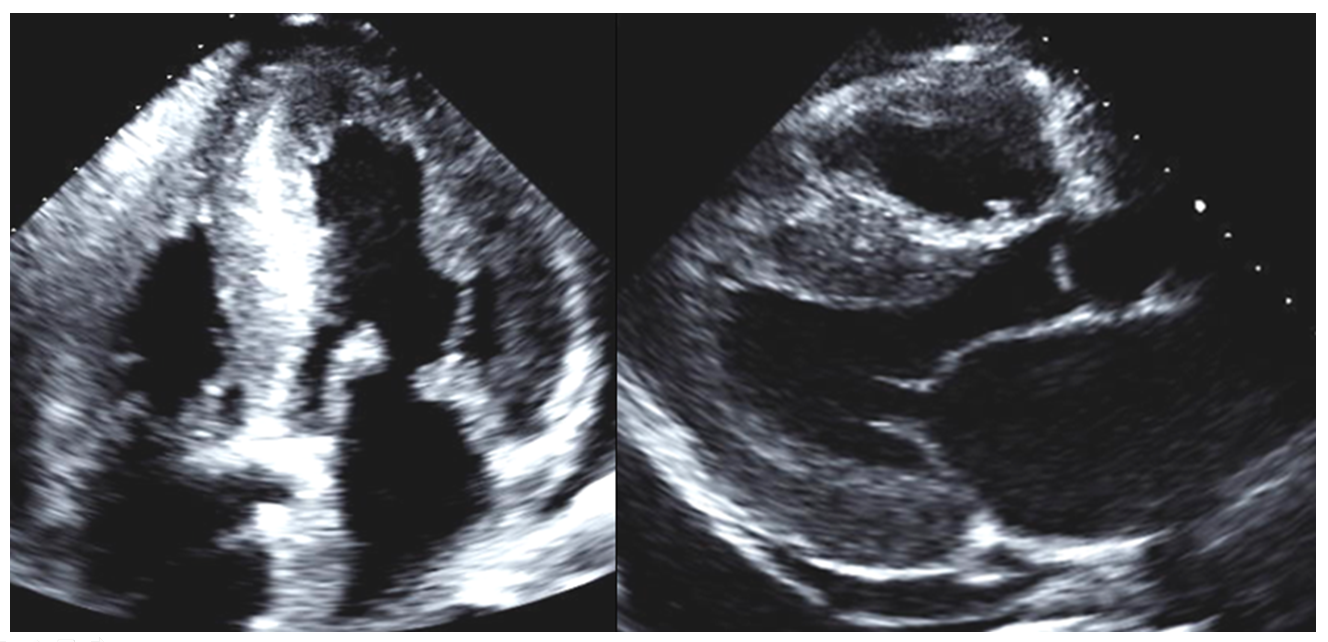
A 49-year-old previously healthy man presents to a hospital with progressive shortness of breath, postural syncope, and palpitations. An echocardiogram reveals severe global left ventricular hypertrophy (Figure 1). Physical examination is remarkable for periorbital purpura, orthostatic hypotension, and signs of heart failure including elevated jugular venous pressure, rales over both lung bases and peripheral pitting edema. His echocardiogram and electrocardiogram (ECG) are shown (Figures 1 and 2). Amlodipine, lisinopril and diuretics are initiated for a presumed diagnosis of hypertensive cardiomyopathy.
Figure 1
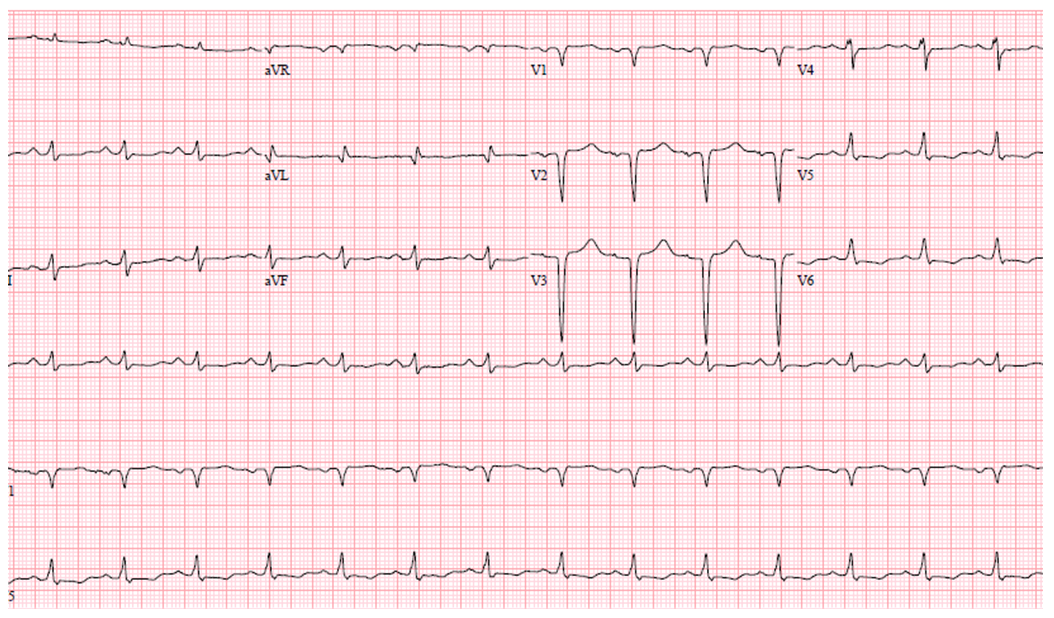
Figure 2
Based on the clinical presentation and objective data, which of the following is correct?
Show Answer
The correct answer is: C. Workup for an infiltrative process should be performed.
An inverse relationship between low ECG voltage and left ventricular (LV) hypertrophy by echocardiogram is an important clue of infiltrative cardiomyopathy in this case. The differential diagnosis for infiltrative disorders, which may result in inappropriately small voltage ECG in an apparently hypertrophic LV due to extracellular substance deposit and myocyte damage, includes cardiac amyloidosis, Fabry disease, Danon disease, mucopolysaccharidoses, myocardial oxalosis or Friedreich ataxia.1 Among these, cardiac amyloidosis is the most prevalent condition, and would explain symptoms observed in this case. The peripheral and autonomic nerves and skin involvement strongly suggest AL amyloidosis, a plasma cell disorder that produces excessive monoclonal immunoglobulin light chains. This abnormal protein deposits in extracellular spaces, preferably involving the nervous system, skin, kidneys and heart. Patients with AL amyloidosis are sensitive to afterload reduction due to peripheral and autonomic neuropathy. Fragile skin capillaries resulting from amyloid protein deposition causes periorbital purpura.
The inappropriately low voltage ECG defined as QRS voltage amplitude ≤0.5 mV in all limb leads or ≤1.0 mV in all precordial leads found in ~50-70% of patients with a biopsy-proven cardiac amyloidosis.2,3 Approximately half of the patients also have pseudo-infarction pattern, despite an absence of significant epicardial coronary artery disease.2,3 This finding is thought to be from microvascular invasion, resulting in myocyte atrophy and myocardial fibrosis. Amyloid can infiltrate the atria as well as the ventricles, and may cause atrial dysfunction which predispose to atrial thrombi and atrial fibrillation found in 10-15%.3,4 Cardiac amyloidosis is also associated with ventricular arrhythmias and sudden cardiac death. This patient was admitted for treatment of heart failure and underwent bone marrow biopsy, which proved AL amyloidosis.
References
Seward JB, Casaclang-Verzosa G. 2010. Infiltrative cardiovascular diseases: cardiomyopathies that look alike. J Am Coll Cardiol. 2010;27:1769-79.
Rahman JE, Helou EF, Gelzer-Bell R, Et al. Noninvasive diagnosis of biopsy-proven cardiac amyloidosis. J Am Coll Cardiol 2004;43:410-5.
Cheng Z, Zhu K, Tian Z, Zhao D, Cui Q, Fang Q. The findings of electrocardiography in patients with cardiac amyloidosis. Ann Noninvasive Electrocardiol 2013;18:157-62.
Murtagh B, Hammill SC, Gertz MA, Kyle RA, Tajik AJ, Grogan M. Electrocardiographic Findings in Primary Systemic Amyloidosis and Biopsy-Proven Cardiac Involvement. Am J Cardiol 2005;95:535-7.