A 78-year-old male with osteoarthritis, depression, dyslipidemia, and inferior myocardial infarction (MI) s/p right coronary artery (RCA) stenting two years ago presents to your office for initial consultation. An additional problem is that the patient has hypertension with systolic blood pressures (SBPs) in the 150-155 mm Hg range, based on home and clinic readings, despite a low-sodium diet and moderate exercise. He walks three times per week for one hour without angina or limiting dyspnea. His medications include atenolol 50 mg daily, atorvastatin 10 mg daily, and aspirin 81 mg daily. He has been compliant with his drug regimen, and he denies orthostatic dizziness or significant lower extremity edema.
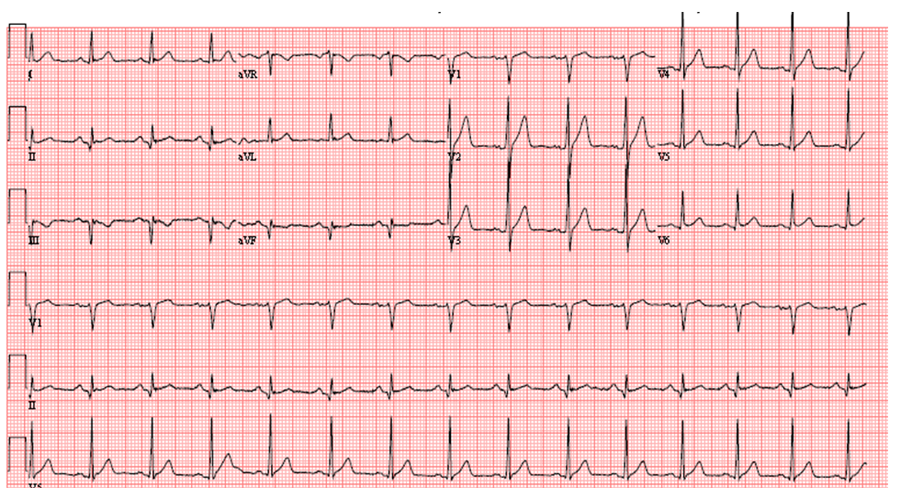
Figure 1
On physical exam his brachial blood pressure (BP) is 150/70 mm HG on the left and 153/72 mm HG on the right, and pulse 70 beats per minute (bpm). There is no fall in BP after standing for one minute. He appears well. There is mild thinning of hair on his anterior tibial surfaces, and extremities are warm with 2+ distal pulses. His cardiac exam is notable for a soft S4 and 2/6 systolic ejection murmur at the base. Combined with normal carotid upstrokes and a normal S2, the murmur is most consistent with aortic valve sclerosis. The remainder of the exam is normal. A recent lab panel shows a normal creatinine of 0.8 mg/dL, normal electrolytes, and low-density lipoprotein cholesterol (LDL-C) of 78 mg/dL.
His electrocardiogram (ECG) (Figure 1) reveals normal sinus rhythm with a rate of 80 bpm, normal axis and intervals, and evidence of prior inferior MI, but no apparent left ventricular hypertrophy.
In addition to reinforcing a low-sodium diet and moderate exercise, which of the following is the next best step in the management of his hypertension?
Show Answer
The correct answer is: B. Add lisinopril 2.5 mg PO daily.
We would suggest that in a relatively fit elderly patient population with a history of MI or obstructive coronary artery disease (CAD), the first drug of choice for hypertension would be an angiotensin-converting enzyme inhibitor (ACEI), and the goal BP should certainly be less than 150 mm Hg. Based on Eight Joint National Committee (JNC 8) guidelines, patients ≥60 years of age are candidates for pharmacologic therapy if the SBP is ≥150 mm Hg or diastolic blood pressure (DBP) is ≥90 mm Hg, and the goal BPs are <150 mm Hg and <90 mm Hg, respectively.1 The goals are <140 mm Hg and <90 mm Hg if chronic kidney disease (CKD) or diabetes is present. Given these recommendations, answer option E is not the best choice. The JNC 8 guidelines recommend initiating a thiazide diuretic, or ACEI or angiotensin-receptor blocker (ARB), or Ca2+ channel blocker (CCB) for non-black patients ≥60 years of age, either alone or in combination. This patient has stable ischemic heart disease (SIHD), and based on a Class I recommendation from the ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with SIHD, an ACEI is recommended as the best antihypertensive medication for this patient with SIHD.2 Thus, answer option A is not the best choice; also, note that the initial dose of chlorthalidone should be 12.5 mg daily, especially in elderly patients at greater risk of low BP and hyponatremia as the result of lower intravascular volume and renal blood flow compared to younger patients.1 While the combination therapy in answer option C is listed in the JNC 8 guidelines as an acceptable strategy to dose antihypertensive medications, a more conservative strategy is suggested in this elderly patient at greater risk from complications of low BP.1 A strategy of starting low doses of antihypertensive drugs with a gradual lowering of BP is recommended. Answer option D is not the best answer as potential side effects from increasing the beta-blocker dose include fatigue; in addition, the JNC 8 guidelines do not recommend beta-blockers for the initial treatment of hypertension because of data suggesting a higher risk of stroke compared to other antihypertensive drugs.1 Based on these principles, the authors of this case consider answer option B to be the best choice.
What is the Goal BP in This Patient?
In the JNC 8 guidelines, the recommendation is to reduce SBP to less than 150 mm Hg in the elderly without CKD or diabetes.1 However, post-hoc analysis from the International Verapamil-Trandolapril (INVEST) study, a comparison of two antihypertensive regimens in patients with ischemic heart disease and age ≥60 years, showed that cardiovascular outcomes were improved in patients with SBP <140 mm Hg, when compared to patients with SBP 140-<150 mm Hg.3 Although this post-hoc data does not provide convincing evidence of benefit from the lower BP goal, it certainly appears to be safe to lower the SBP to < 140 mmHg in elderly patients with ischemic heart disease. The JNC 8 guidelines do recommend that medical therapy not be adjusted in elderly patients with SBP <140 mm Hg, as long as the therapy did not have "adverse effects on health or quality of life."1 Given the potential for a "J-curve" effect on mortality, it is reasonable to keep the diastolic blood pressure (DBP) above 60-65 mm Hg, but there is no lower limit for DBP recommended by the ESC/ESH and JNC 8 guidelines.1,4
References
James PA, Oparil S, Carter BL, et al. 2014 evidence based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014;311:507-20.
Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2012;60:2564-603.
Bangalore S, Gong Y, et al. 2014 Eighth Joint National Committee panel recommendation for blood pressure targets revisited: Results from the INVEST study. J Am Coll Cardiol 2014;64:784-93.
Mancia G, Fagard R, Narkiewicz K, et al. 2013 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013;31:1281-357.