A 45-year-old Caucasian male is seen in clinic complaining of shortness of breath. He has a history of heart failure with reduced ejection fraction (HFrEF) secondary to coronary artery disease and is status post 3-vessel coronary artery bypass graft (CABG) surgery along with percutaneous coronary intervention to the right posterior descending artery. A recent echocardiogram demonstrated improvement in his ejection fraction from 15% to 25% after cardiac resynchronization therapy and defibrillator (CRT-D) implantation. The repeat echocardiogram continued to show mild LV dilatation with antero-apical akinesis. Nuclear stress test did not demonstrate any area of reversible ischemia. A sleep study was performed and the patient was started on continuous positive airway pressure. He is on appropriate guideline-directed medical therapy that includes carvedilol 37.5mg PO BID, losartan 100mg PO daily, spironolactone 25mg PO daily, and furosemide 40mg twice a day. A physical exam did not demonstrate evidence of volume overload. He was then sent for a functional VO2 study that revealed a good exercise capacity with a peak VO2 of 21 mL/kg/min. Despite this, he continued to have dyspnea with New York Heart Association (NYHA) functional class III symptoms.
Which of the following is the next step you should consider?
Show Answer
The correct answer is: B. LV partitioning device placement.
Several points highlight choice B as the best option. First, referring the patient for an LVAD or heart transplantation can be considered, but as the patient recently demonstrated a peak VO2 of >14 mL/kg/min on his functional VO2 study, he currently does not meet one of the indications for such a treatment strategy. Echocardiogram guided bi-ventricular pacing optimization may be more useful in those patients who are non-responders to cardiac resynchronization therapy. We know that myocardial infarction (MI), especially in the left ventricular antero-apical region, leads to a remodeling process with an increase in left ventricular volume that has been associated with a poor clinical outcome. Current management intends to reverse the remodeling process by medical and cardiac implanted electrical device based therapy. This patient has undergone CRT and is optimized on guideline-directed medical therapy, despite this, he continues to have New York Heart Association functional class III symptoms. Surgical techniques known as surgical ventricular restoration have historically attempted to restore the LV. The Surgical Treatment for Ischemic Heart Failure (STITCH) trial was met with mixed results. With operative risks in mind, percutaneous ventricular restoration (PVR) or a catheter-based approach was developed. The PARACHUTE trials have looked at the feasibility of such a procedure. An LV partitioning device known as Parachute™ (CardioKinetix, Inc., Menlo Park, California) is deployed percutaneously into the LV in patients with antero-apical wall motion abnormalities. This aims to exclude the infarcted akinetic or dyskinetic regions and restore the internal LV geometry by reducing intracardiac volume and optimizing ventricular wall stress. Thus far, patients have demonstrated clinical benefit with improvement in NYHA functional class and a trend towards improvement in quality of life. Currently the PARACHUTE IV trial is enrolling patients to study the safety and efficacy of PVR using this device versus optical medical therapy. This patient underwent PVR with this device and upon 3–6 month clinic follow-up reports NYHA functional class I-II symptoms. It should be noted that although this device is still investigational, it nonetheless represents a new frontier in interventional or a catheter-based approach for treatment and management of patients with ischemic cardiomyopathy and HFrEF.
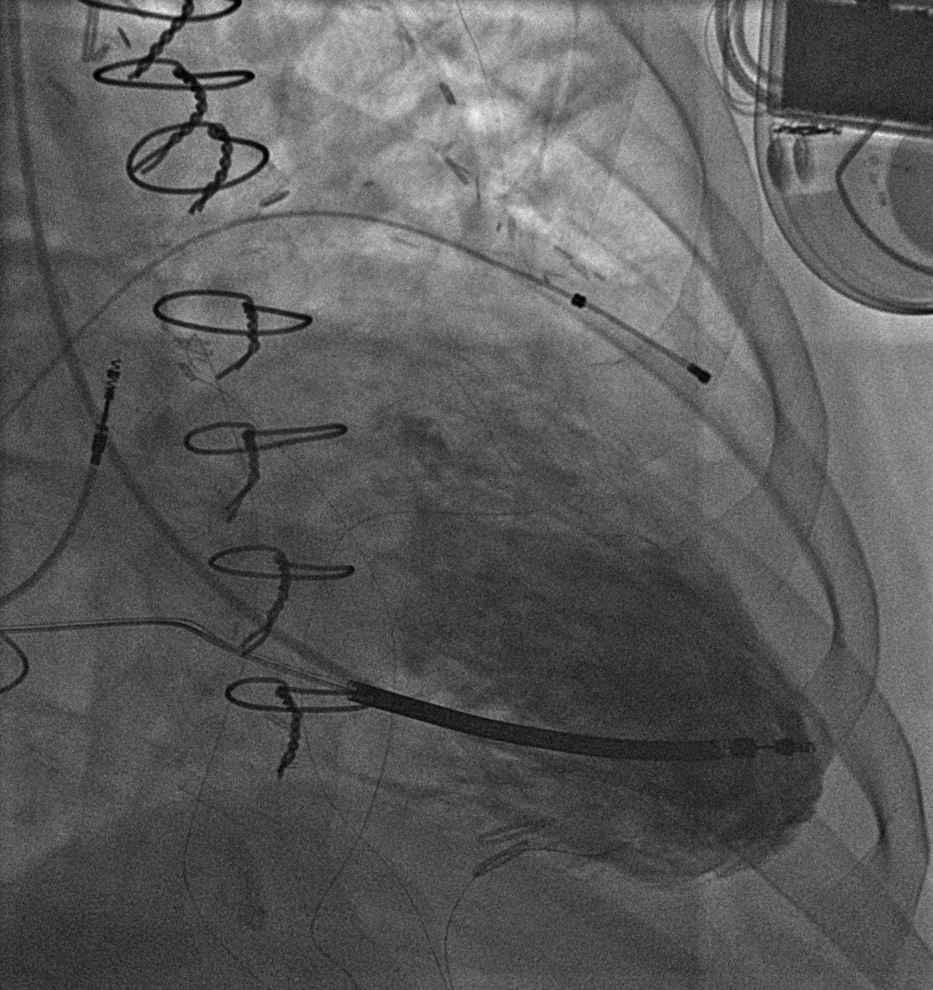
Figure 1: Left Ventriculogram Pre-LV Partitioning Device Deployment
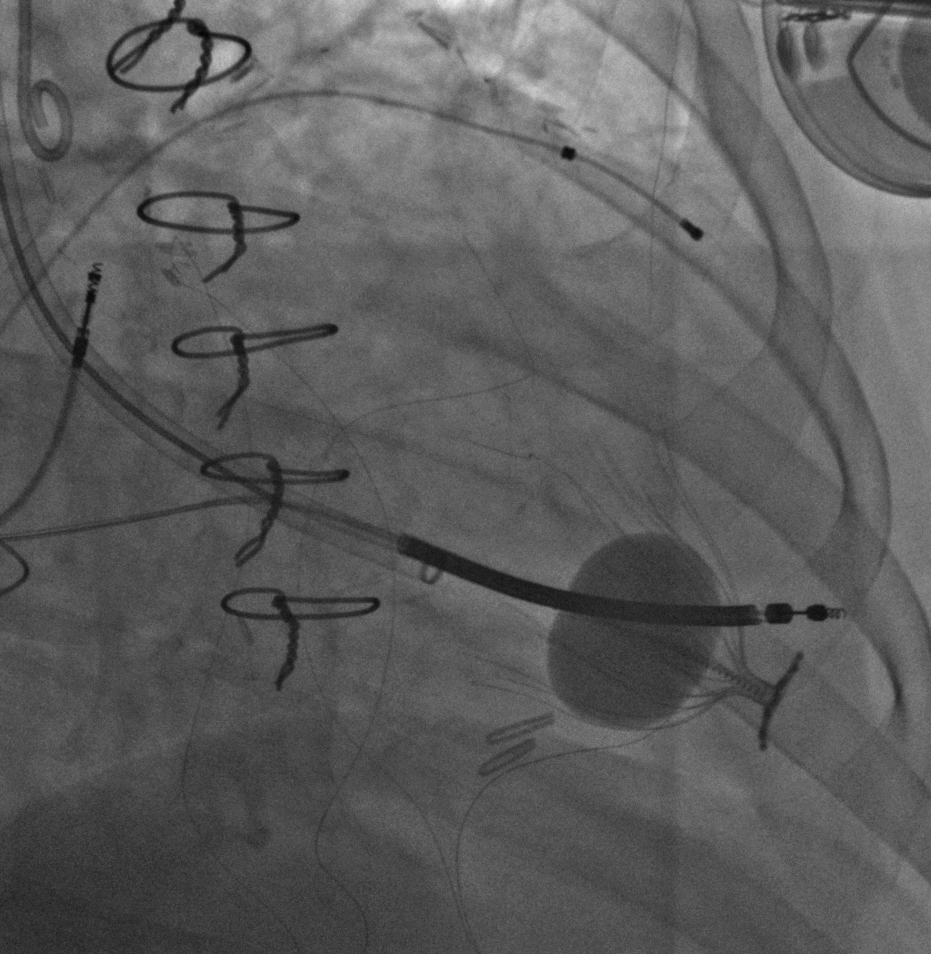
Figure 2: LV Partitioning Device During Deployment
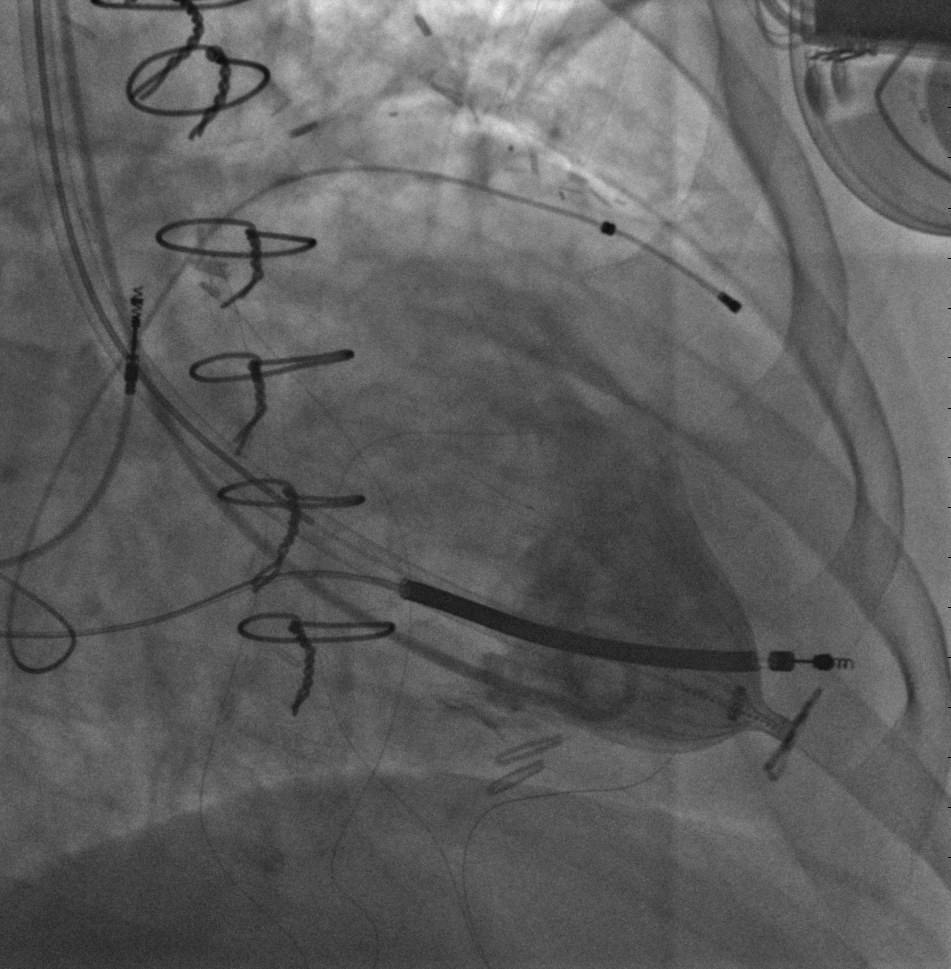
Figure 3: Left Ventriculogram Post-LV Partitioning Device Deployment
References
Costa MA, Pencina M, Nikolic S, Engels T, Templin B, Abraham WT. The PARACHUTE IV trial design and rationale; percutaneous ventricular restoration using the parachute device in patients with ischemic heart failure and dilated left ventricles. Am Heart J 2013;165:531-6.
Mazzaferri EL, Gradinac S, Sagic D, et al. Percutaneous left ventricular partitioning in patients with chronic heart failure and a prior anterior myocardial infarction: results of the percutaneous ventricular restoration in chronic heart failure patients trial. Am Heart J 2012;163:812-20.
Costa MA, Mazzaferri EL, Sievert H, Abraham WT. Percutaneous ventricular restoration using the parachute device in patients with ischemic heart failure: three-year outcomes of the PARACHUTE first-in-human study. Circ Heart Fail 2014;7:752-8.
Bozdag-Turan I, Bermaoui B, Paranskaya L, et al. Challenges in patient selection for the parachute device implantation. Catheter Cardiovasc Interv 2013;82:E718-25.
Ige M, Al-Kindi SG, Attizzani G, Costa M, Oliveira GH. Percutaneous left ventricular restoration. Heart Fail Clin 2015;11:261-73.
Fang F, Liu W, Zhao YX, et al. The patient's selection of PARACHUTE® endoventricular partitioning device: the important role of detailed echocardiography. Int J Cardiol 2015;195:176-9.
Cilingiroglu M, Rollefson WA, Mego D. Percutaneous implantation of a parachute device for treatment of ischemic heart failure. Cardiovasc Revasc Med 2013;14:236-40.
Nikolic SD, Khairkhahan A, Ryu M, Champsaur G, Breznock E, Dae M. Percutaneous implantation of an intraventricular device for the treatment of heart failure: experimental results and proof of concept. J Card Fail 2009;15:790-7.
Stone PH, Raabe DS, Jaffe AS, et al. Prognostic significance of location and type of myocardial infarction: independent adverse outcome associated with anterior location. J Am Coll Cardiol 1988;11:453-63.
Mancini D, Lietz K. Selection of cardiac transplantation candidates in 2010. Circulation 2010;122:173-83.
Gage RM, Burns KV, Vatterott DB, Kubo SH, Bank AJ. Pacemaker optimization in nonresponders to cardiac resynchronization therapy: left ventricular pacing as an available option. Pacing Clin Electrophysiol 2012;35:685-94.