A 52-old-man was referred by his internist for complaints of worsening exertional chest pain and shortness of breath of two months duration. He had no previous history of coronary artery disease, but had hypertension, hyperlipidemia, diabetes, morbid obesity with a body weight of 360 pounds and sleep apnea treated with continuous positive airway pressure (CPAP). He had undergone knee surgery for degenerative arthritis. He was a non-smoker. He was currently treated with aspirin (81 mg qd), metoprolol (50 mg bid), amlodipine (10 qd) and atorvastatin (40 qd). He also wants to have bariatric surgery.
His resting electrocardiogram (ECG) was normal. A pharmacologic exercise tolerance test revealed a large area of inferolateral ischemia. He was loaded with 600 mg clopidogrel and given instructions to take 75 mg daily in anticipation of the need for percutaneous coronary intervention (PCI) and underwent elective coronary angiography. His angiogram is shown in Videos 1, 2 and 3. There was a high grade, hazy, approximate 75% stenotic lesion in the mid circumflex AV groove segment (Video 1) and a 75% stenosis in the distal right coronary artery (RCA) right before the patent ductus arteriosis (PDA) takeoff (Video 2). There was also a concerning approximate 75% stenosis in the mid-left anterior descending artery (LAD) (Video 3).
His case was presented to the cardiac surgery team who felt that the patient was a poor candidate for coronary artery bypass graft (CABG) due to morbid obesity. Moreover, there was no objective evidence of ischemia in the LAD distribution on perfusion imaging. The decision was made to proceed with PCI of the circumflex and RCA lesions and to perform fractional flow reserve (FFR) in the LAD.
This patient has demographic variables associated with clopidogrel resistance (morbid obesity, diabetes, non-smoking status) and is now to undergo multivessel, and possibly three-vessel, stenting.
Would you perform platelet function testing on this high-risk patient?
Show Answer
The correct answer is: B. Yes, to ensure that there is an adequate pharmacodynamic response from clopidogrel before multiple stent implantation in this high-risk patient.
Pharmacodynamic studies have clearly demonstrated wide response variability with non-responsiveness or high on-treatment platelet reactivity to adenosine diphosphate (ADP) (high platelet reactivity [HPR]) in about one third of patients treated with clopidogrel who have undergone PCI. It is well established that HPR during clopidogrel therapy is an independent risk factor for ischemic event occurrence in post-PCI patients.1,2 There is a Class IIb recommendation that platelet function testing may be considered in patients at high risk for poor clinical outcomes.3
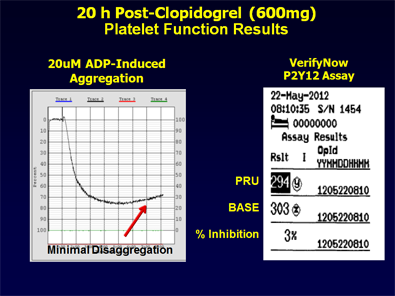
Figure 1
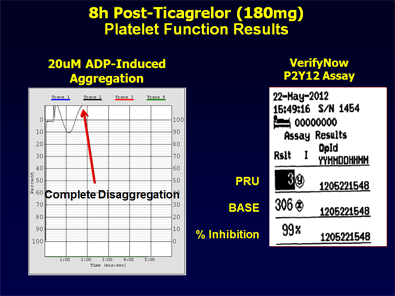
Figure 2
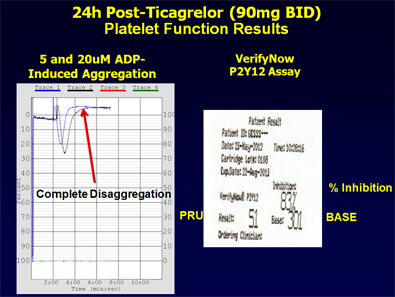
Figure 3:
At this time, there is no evidence from large-scale prospective trials that personalization of antiplatelet therapy based on platelet function testing improves post-PCI clinical outcomes. However, there are limitations to the two main negative trials that were conducted. Importantly, patient risk was overall low and the regimen to overcome clopidogrel resistance was primarily a doubling of the standard clopidogrel dose. The latter regimen has been found to be pharmacodynamically ineffective in overcoming resistance in about 40% of patients.1,2
On-treatment platelet reactivity was measured with conventional aggregometry (ADP-induced platelet aggregation) and VerifyNow P2Y12 assay. The patient was found to be resistant to clopidogrel and had HPR (Figure 1).
The patient was loaded with 180 mg ticagrelor, a P2Y12 inhibitor with a more potent and rapid antiplatelet response compared to clopidogrel.4
Platelet function testing was again performed 8 hours and 24 hours after 180 mg ticagrelor loading dose + 90 mg BID maintenance dose, and results appear in Figures 2 and 3.
PCI was successfully performed the day following the start of ticagrelor therapy with DES in the circumflex (3.5 x 12 mm Resolute) and RCA (2.5 x 18 mm Resolute). Post-stent angiograms are shown in Videos 4 and 5. FFR of the LAD was 0.93.
The patient was discharged on aspirin (81 mg qd) and ticagrelor (90 mg bid) in addition to his prior medical regimen.
References
Tantry US, Bonello L, Aradi D, Gurbel PA et al. Working Group on On-Treatment Platelet Reactivity. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding. J Am Coll Cardiol 2013;62:2261-73.
Gurbel PA, Tantry US. Do platelet function testing and genotyping improve outcome in patients treated with antithrombotic agents?: platelet function testing and genotyping improve outcome in patients treated with antithrombotic agents. Circulation 2012;125:1276-87.
Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011;58:e44-122.
Gurbel PA , Bliden KP , Butler KD, et al. Randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease: the ONSET/OFFSET study. Circulation 2009;120:2577-2585.