Patient 1:
A 70-year-old Caucasian man with multiple chronic conditions/multimorbidity,1,2 without a prior history of stroke or TIA, body mass index of 26 kg/m2 (77 kg) presents with angina pectoris and a surface ECG showing anterior ST-elevation myocardial infarction (STEMI). While obtaining a focused medical history, in preparation for transport to the cardiac catheterization laboratory, he and his family state that he has been slowing down (having trouble crossing a street in the allotted time, low overall physical activity, weight loss over the past year). He is transported to the cardiac catheterization where a drug eluting stent is placed across the proximal left anterior descending artery.
Patient 2:
A 76-year-old Hispanic man with multimorbidity,1 without a prior history of stroke or TIA, body mass index of 26 kg/m2 (77 kg) presents with angina pectoris and a surface ECG showing anterior ST-elevation myocardial infarction (STEMI). While obtaining a focused medical history, in preparation for transport to the cardiac catheterization laboratory, he and his family are surprised that he is having a heart attack. Prior to this, they state he has been physically active playing doubles tennis 4-5 times a week, and golfing once a week. He is transported to the cardiac catheterization where a drug eluting stent is placed across the proximal left anterior descending.
At the end of the procedure you are deciding between prasugrel or clopidogrel as an optimal antiplatelet therapy. You remember that the drug monograph states that prasugrel is generally not recommended in patients over 75 year of age.
Regarding a continuous variable such as chronological age (or weight) which of the following statements is FALSE?
Show Answer
The correct answer is: B. Grouping a continuous variable into age categories (deciles, quintiles, or others) assumes that there is a variation of risk across the categories.
Answer A is true. Royston, Altman, and Sauerbrei clearly point to the problems associated with dichotomizing continuous variables such as age.3-5 Loss of information is one large problem associated with this method. The other is increasing the type I error rate (false-positive). The STRengthening Analytical Thinking for Observational Studies: STRATOS initiative points to the importance of this topic.6
Answer B is false and is the correct answer. Grouping of ages into categories brings up issues of multiple hypothesis testing and difficulty comparing varying cut-points between studies. An important clinical point to remember is that categorization assumes that there is equal risk across categories.5-7
Answer C is true. The definition of elderly or "older adults" can vary and is currently based on an arbitrary chronological age cutoff or age categories. The World Health Organization's (WHO) defines age as a binary variable (>60 years of age). Another commonly used definition categorizes chronological age into "young old" (60-74 years), "old old" (75-84 years), and "very old" (≥ 85 years).
There is currently no single method in determining physiological age. Geriatric cardiologists often address physiological age phenotypically using chronological age, along with concepts of multimorbidity, disability, frailty, etc. Age scaling of comorbidities may improve on this in the future.8
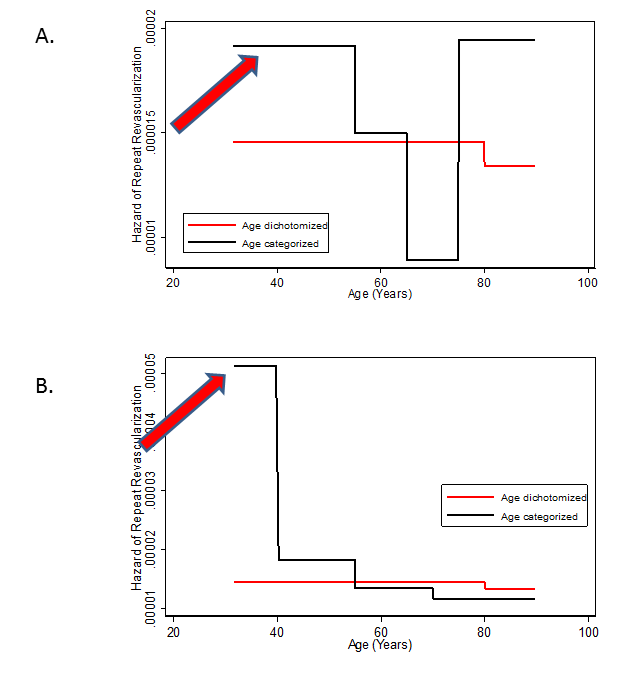
Answer D is true. In a sensitivity analysis, it was demonstrated that arbitrary changes in age categories can result in a different and opposite interpretations in the association between age and repeat coronary revascularization in patients with end stage renal disease (Figure 1).7
Answer E is intuitively true. Chronological age is known to be associated with outcomes such as mortality. The strength of this association varies often based on the presence or absence of a dominant comorbidity or the presence of multimorbidity.9,10
Overview
The known pitfalls of breaking up a continuous variable, such as age in the current example, are not novel and have been in the statistical literature for approximately two decades. The authors do not recommend the use of prasugrel in contradiction to the current drug monograph. This case example was used to illustrate that clinicians are often asked to base a decision on an age cutoff. This case example also points to a younger, perhaps slightly more frail, individual possibly being prescribed prasugrel while an older, perhaps slightly less frail, individual probably not prescribed prasugrel based purely on an age cutoff. Furthermore, there are currently no clinical prediction models (risk scores) that are available to determine the benefit versus bleeding risk of prescribing prasugrel in comparison to other dual antiplatelet therapies after percutaneous coronary intervention. Currently, the decision to prescribe prasugrel should proceed based on the drug manufacturer's recommendations until more information is available.
Lastly, it is important to point to recent changes in how we describe aging in individuals: "Descriptive terms for older people: older is in and elderly is out."11
Figure 1: Two standard modeling strategies for the continuous variable age as a function of repeat revascularization in the fit of an unadjusted parametric survival regression.
A. Orange solid line = age dichotomized at 80 years; Black solid line= age categorized (<55, 55-64, 65-74, & ≥75 years) B. A sensitivity analysis is shown with a change in the age category (Black solid line) when a small change in the age category is made (<40, 40-54, 55-69, & ≥70 years). The red arrows demonstrate graphically the changes in interpretation with change in age categories.
Adapted with permission from Krishnaswami et al.7
Vogeli C, Shields AE, Lee TA, et al. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs. J Gen Intern Med 2007;22:391-5.
Royston P, Altman DG, Sauerbrei W. Dichotomizing continuous predictors in multiple regression: a bad idea. Stat Med 2006;25:127-41.
Altman DG, Lausen B, Sauerbrei W, Schumacher M. Dangers of using "optimal" cutpoints in the evaluation of prognostic factors. J Natl Cancer Inst 1994;86:829-35.
Bennette C, Vickers A. Against quantiles: categorization of continuous variables in epidemiologic research, and its discontents. BMC Med Res Methodol 2012;12:21.
Sauerbrei W, Abrahamowicz M, Altman DG, le Cessie S, Carpenter J, STRATOS initiative. STRengthening analytical thinking for observational studies: the STRATOS initiative. Stat Med 2014;33:5413-32.
Krishnaswami A , Forman DE, Leong TK, Go AS, McCulloch CE. Association of age with mortality and repeat revascularization in end-stage renal disease patients. Perm J 2016;20:4-9.
Normand SL, Morris CN, Fung KS, McNeil BJ, Epstein AM. Development and validation of a claims based index for adjusting for risk of mortality: the case of acute myocardial infarction. J Clin Epidemiol 1995;48:229-43.
Krishnaswami A, Kiley ML, Anthony FF, et al. Effect of advancing age and multiple chronic conditions on mortality in patients with end-stage renal disease after implantable cardioverter-defibrillator placement. Perm J 2016;20:27-32.
Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care 2006;29:725-31.