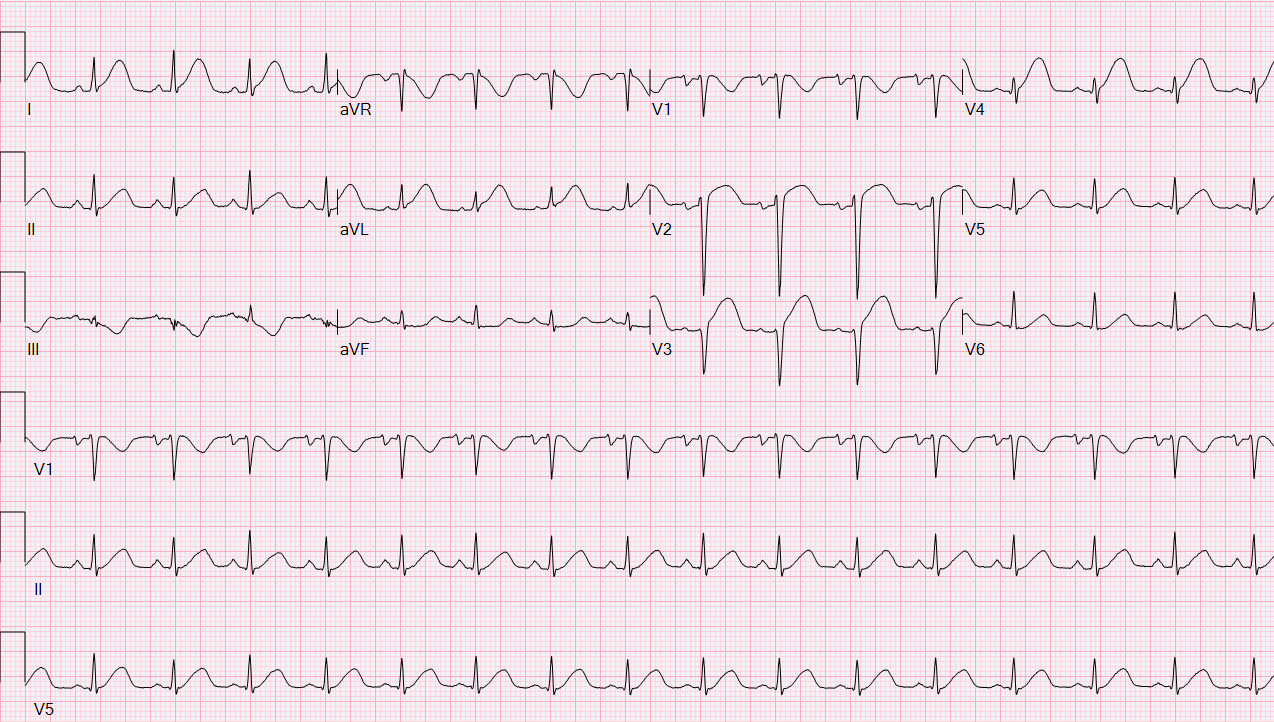
A 32-year-old pregnant (G9P4) African-American woman at 38 weeks of gestation presented with acute-onset substernal chest pain radiating to her left shoulder, accompanied by dyspnea and diaphoresis. Her past medical history was significant for well-controlled bronchial asthma. She was hemodynamically stable at the time of her presentation. Her initial 12-lead electrocardiogram demonstrated anterior ST-segment elevation (Figure 1). Bedside echocardiography in the emergency department revealed hypokinesis in the mid- to distal-anterior, distal septal, and apical walls of the left ventricle, with an ejection fraction of 30-35% (Video 1). She was started on aspirin, a statin, nitroglycerin, and intravenous unfractionated heparin. After emergent consultation from obstetrics, cardiothoracic surgery, and pediatrics, a decision was made to take her for coronary angiography. Angiography revealed spontaneous coronary artery dissection involving the mid-portion of the left anterior descending artery (LAD) with a large intramural hematoma extending from the proximal third of the LAD and sparing of the distal portion of the artery, which had Thrombolysis in Myocardial Infarction-3 flow (Videos 2-3).
Figure 1: 12-L Electrocardiogram on Admission Showing ST-segment Elevation in Anterior Precordial Leads
Video 1
Transthoracic echocardiogram on admission showing hypokinesis in the mid- to distal-anterior, distal septal, and apical walls of the left ventricle, with an ejection fraction of 30-35%.
Video 2: Coronary Angiogram on Admission
Right anterior oblique (RAO) caudal projection showing spontaneous coronary artery dissection involving the mid-portion of the LAD.
Video 3: Coronary Angiogram on Admission
RAO cranial projection showing spontaneous coronary artery dissection involving the mid-portion of the LAD.
Which one of the following statements is correct regarding the best management option for this patient?
Show Answer
The correct answer is: C. Defer stenting or thrombolysis of the culprit LAD lesion. Continue medical management with aspirin and nitroglycerin. Assess for spontaneous healing of the coronary artery dissection after 4 weeks either by coronary angiogram or optical coherence tomography.
This patient presented with ST-segment elevation myocardial infarction and presumably new left ventricular dysfunction due to spontaneous coronary artery dissection involving the proximal to mid-LAD.
Spontaneous coronary artery dissection refers to the spontaneous separation of the coronary arterial wall that is non-iatrogenic, non-traumatic, and non-atherosclerotic in origin. Although once considered rare due to limited diagnostic capabilities, it is now recognized as a pertinent differential diagnosis in young women presenting with chest pain. Pregnancy-associated spontaneous coronary artery dissection is a distinct type of spontaneous coronary artery dissection that is the most frequent cause of pregnancy-related myocardial infarction.1 It can occur antepartum or postpartum.
The pathogenesis of spontaneous coronary artery dissection is thought to be due to either an intimal tear initiating arterial wall separation or spontaneous bleeding into the arterial wall from increased density of the vasa vasorum. In both instances, a false lumen is created in the culprit artery, which then causes compression of the true lumen, leading to myocardial ischemia and subsequent infarction.2 In the case of pregnancy-associated spontaneous coronary artery dissection, the hormonal and hemodynamic changes associated with pregnancy are thought to be contributory. High progesterone levels during pregnancy weaken the arterial media by altering the elastic fiber and mucopolysaccharide content along with impaired collagen synthesis. The augmented cardiac output and circulating blood volume during pregnancy and increased abdominal wall pressure during labor all contribute to increased arterial wall shear stress that can precipitate pregnancy-associated spontaneous coronary artery dissection. Multiple pregnancies can lead to chronic repetitive impairment of arterial wall integrity, making her at higher risk for spontaneous coronary artery dissection, as was possibly the case with this multiparous patient.
The first important point to take away from this case is that there are no randomized trials comparing medical therapy from revascularization strategies (PCI, CABG) in acute coronary syndromes (ACS) due to spontaneous coronary artery dissection, unlike ACS from coronary atherosclerotic disease. Hence, current recommendations on management are largely based on expert opinions drawn from observational series.
The second point to take away from this case is that an overall conservative approach is preferred over revascularization strategies based on observations that arteries involved in spontaneous coronary artery dissection heal spontaneously in most cases and that revascularization, either with PCI/stenting or by means of thrombolysis, is associated with high failure rates. In three prospective series in which repeat coronary angiograms were performed, spontaneous angiographic healing was observed in a combined 85% (151/177) of cases.3-5 In most cases, resorption of intramural hematoma appears to start within days of the dissection, and complete vessel healing usually takes about 1 month. Success rates for PCI for spontaneous coronary artery dissection range from 47-72.5%.3,4,6 PCI for spontaneous coronary artery dissection is associated with the risk of propagating the intramural hematoma anterograde or retrograde, thereby extending the dissection flap. Subacute and late strut malapposition brought about by the natural resorption of the intramural hematoma may also occur over time. The latter increases the risk of stent thrombosis. Finally, spontaneous coronary artery dissections are usually extensive and involve the distal coronary segments that are too small for stent placement. Nevertheless, PCI is appropriate in a small proportion of patients who present with ongoing or recurrent ischemia, hemodynamic instability, ventricular arrhythmias, or left main involvement and who have suitable coronary anatomy. Emergent CABG should be considered for patients with left main dissections, extensive dissections involving proximal arteries, or in patients in whom PCI failed or who are not anatomically suitable for PCI. However, long-term results with CABG appear suboptimal, with reported graft patency of only 27% after a follow-up of 47 months.7 This can be explained by the spontaneous arterial healing with subsequent competitive flow causing graft thrombosis.
The final important teaching point from this case is that guideline-directed medical therapy for ACS such as aspirin, beta-blockade, nitroglycerin, and angiotensin-converting enzyme inhibitor may be beneficial in patients with spontaneous coronary artery dissection. Aspirin, because of its low side-effect profile in ACS and for secondary prevention, appears reasonable to use for both acute and long-term management of spontaneous coronary artery dissection. The use of a second antiplatelet agent such as clopidogrel is of uncertain benefit in those patients with spontaneous coronary artery dissection who were not treated with stents. The latter is usually continued for 12 months post-spontaneous coronary artery dissection and then discontinued once angiographic healing is subsequently demonstrated. Beta-blockers reduce coronary arterial wall stress are thus recommended in the acute and long-term management of spontaneous coronary artery dissection. Nitroglycerin reduces associated coronary artery vasospasm. Angiotensin-converting enzyme inhibitors are recommended in patients with spontaneous coronary artery dissection with significant left ventricular dysfunction. Statins are recommended only in patients with spontaneous coronary artery dissection with pre-existing dyslipidemia. Finally, patients with spontaneous coronary artery dissection should be advised to avoid lifting weights (>20 pounds in women and >50 pounds in men) to have a lower target exercise heart rate and systolic blood pressure during exercise rehabilitation and, in cases of pregnancy-associated spontaneous coronary artery dissection, to avoid future pregnancies.
This patient ultimately underwent cesarean section and delivered a healthy baby girl. Repeat coronary angiography 9 days after her initial presentation showed early spontaneous healing of her coronary artery dissection (Videos 4-5).
Video 4: Coronary Angiogram 9 Days After Presentation
RAO caudal projection showing early spontaneous resolution of the spontaneous coronary artery dissection involving the mid-portion of the LAD.
Video 5: Coronary Angiogram 9 Days After Presentation
RAO cranial projection showing early spontaneous resolution of the spontaneous coronary artery dissection involving the mid-portion of the LAD.
References
Elkayam U, Jalnapurkar S, Barakkat MN, et al. Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation 2014;129:1695-702.
Saw J, Mancini GB, Humphries KH. Contemporary Review on Spontaneous Coronary Artery Dissection. J Am Coll Cardiol 2016;68:297-312.
Tweet MS, Eleid MF, Best PJ, et al. Spontaneous coronary artery dissection: revascularization versus conservative therapy. Circ Cardiovasc Interv 2014;7:777-86.
Saw J, Aymong E, Sedlak T, et al. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv 2014;7:645-55.
Rogowski S, Maeder MT, Weilenmann D, et al. Spontaneous Coronary Artery Dissection: Angiographic Follow-Up and Long-Term Clinical Outcome in a Predominantly Medically Treated Population. Catheter Cardiovasc Interv 2017;89:59-68.
Letierri C, Zavalloni D, Rossini R, et al. Management and Long-Term Prognosis of Spontaneous Coronary Artery Dissection. Am J Cardiol 2015;116:66-73.
Tweet MS, Hayes SN, Pitta SR, et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation 2012;126:579-88.