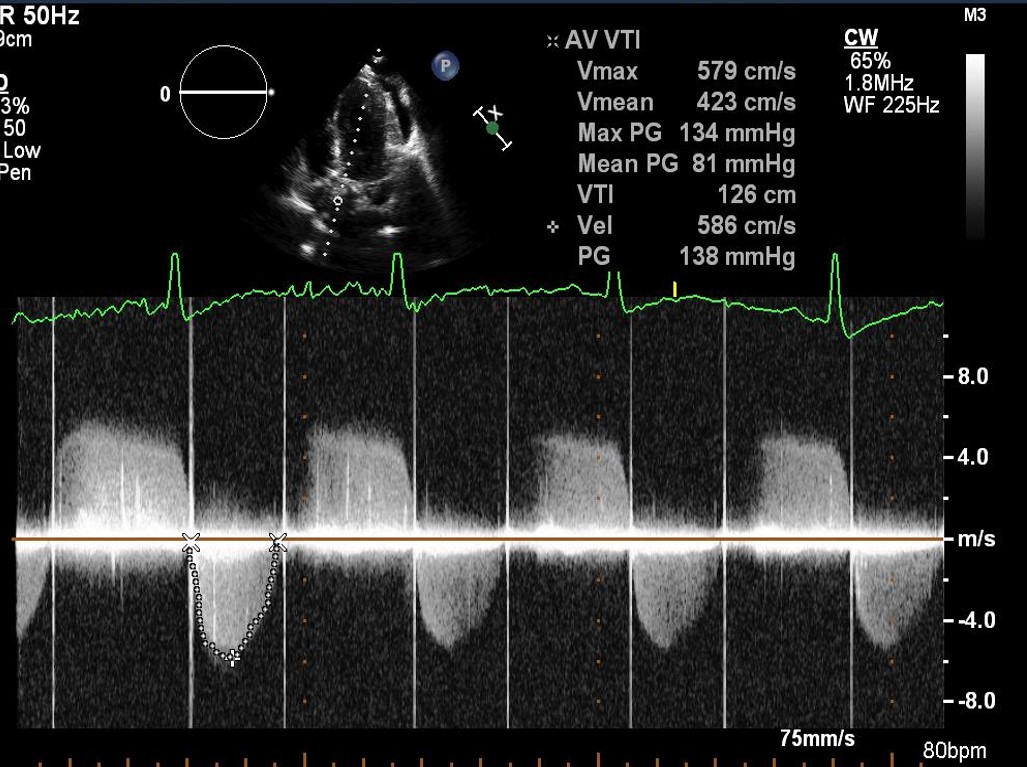
A 19-year-old woman presents with signs and symptoms of heart failure (HF) at 33 weeks gestation of her first pregnancy. The patient was born with truncus arteriosus and underwent ventricular septal defect closure, right ventricle-to-pulmonary artery conduit placement in infancy, with subsequent conduit and mechanical aortic valve replacement as an adolescent. Due to the pregnancy, she was switched from warfarin 10 mg daily to low-molecular-weight heparin at week 6 of gestation. Four months prior to this presentation, while on heparin but with variable compliance, she was hospitalized with a deep venous thrombosis of the right common femoral vein. This was managed conservatively. On this current presentation, she reports 3 weeks of progressive dyspnea on exertion, fatigue, and lower extremity edema that limit her activity. She reports no chest pain, presyncope, syncope, or palpitations. Vital signs are within normal limits. The exam is notable for mild lower extremity edema, a harsh IV/VI systolic ejection murmur at the cardiac base, and a I/IV high-pitched decrescendo diastolic murmur at the apex. Significant laboratory results include 95,000 platelets, B-type natriuretic peptide 273pg/mL, and anti-Xa level 0.62 (goal 0.8-1.2 units/mL). Figures 1 and 2 below are from the transthoracic echocardiogram. Previous baseline aortic valve velocity was 3.8 m/s. A cine clip from aortic valve fluoroscopy is shown in Video 1.
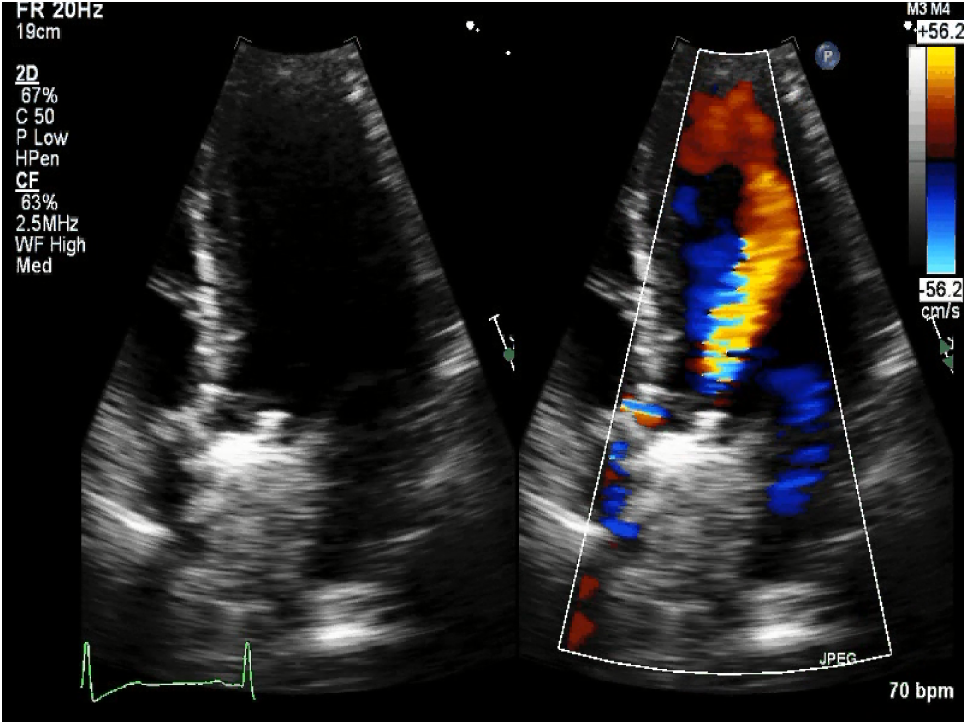
Figure 1: Color Doppler Across the Aortic Valve
Figure 2: Doppler Echocardiography Across the Aortic Valve
Video 1: Aortic Valve Fluoroscopy
What is the next step in this patient's management?
Show Answer
The correct answer is: A. Transesophageal echocardiogram to evaluate for thrombus and thrombus size
The patient's clinical presentation of HF with abnormal valve leaflet motion and acute elevation in aortic valve anterograde velocity suggests valve thrombosis. Although the situation should be considered an emergency that warrants intervention, of chief concern is the viability of her late-stage pregnancy. She is hemodynamically stable, without evidence for cardiogenic shock despite Class III-IV HF symptoms.
According to the 2014 American College of Cardiology/American Heart Association valve guidelines, the next step in management should be transesophageal echocardiography (TEE) to further investigate the possibility of valve thrombosis, particularly to determine thrombus size.1 Computed tomography may be useful initially, either in conjunction with or in place of fluoroscopy, but it is less useful once left-sided prosthetic valve thrombosis is suspected. Emergency valve replacement surgery should be considered, but because the patient is hemodynamically stable, this can be delayed if deemed safe to avoid jeopardizing the viable fetus. Surgical indications via TEE include large thrombus size (0.8 cm2) or finding a mobile thrombus. Fibrinolytic therapy may be considered if the symptoms are recent onset (<14 days), Class I-II, and/or after TEE confirmation of a small, stable thrombus (<0.8 cm2). However, this is not a favorable option for a pregnant woman given the increased risk of bleeding. Transcatheter aortic valve replacement is not an option.
The patient was admitted to the cardiac intensive care unit and immediately started on a continuous infusion of unfractionated heparin. Failure of anticoagulation was thought due to medication nonadherence. Catheter-guided hemodynamic monitoring revealed clinical stability; therefore, the decision was made to proceed with Cesarean section delivery at 34 weeks gestation (6 days after presentation), followed by surgical aortic valve replacement 3 days post-partum. Figure 3 demonstrates the thrombus as seen by TEE. A large thrombus (~2 x 1.5 cm) with pannus was confirmed at the time of explantation.
Figure 3: TEE Image of Thrombus on the Aortic Valve
References
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2438-88.