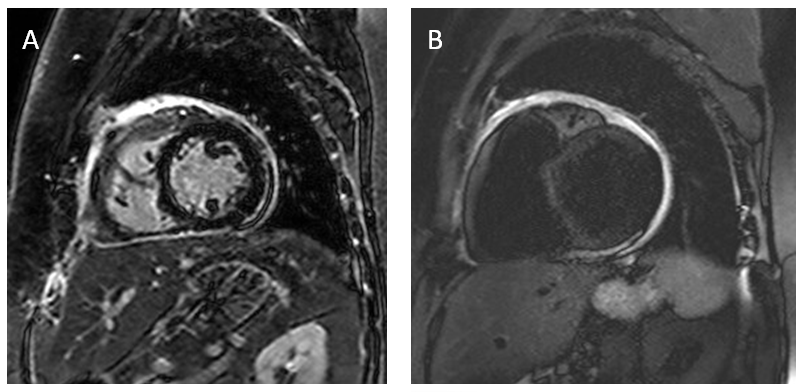
A 53-year-old woman presents with a two-year history of recurrent fever, shortness of breath and an erythematous rash located primarily on the face, neck and upper chest. She also complains of frequent pleuritic chest pain. Review of systems is positive for fatigue, weight gain, joint pain, myalgia, dry eyes and dry mouth, nausea and abdominal pain. The patient denies orthopnea, paroxysmal nocturnal dyspnea, peripheral edema, palpitations or dizziness. Her blood pressure is 138/90 mmHg, temperature is 98.4F, respiratory rate is 14 breaths per minute, with an oxygen saturation of 95%, and heart rate at 72 beats per minute. Physical exam is notable for an obese woman with erythematous patches and plaques on face, chest and trunk. Cardiopulmonary exam is significant for elevated jugular venous pressure at 9 cm H2O, pericardial friction rub and reduced breath sound in the lung bases. The remainder of the exam is within normal limits. A complete blood count is unremarkable. B-type Natriuretic Peptide (BNP) is 271 pg/mL. Westergren sedimentation rate (WSR) and C-reactive protein (CRP) levels are elevated at 39 mm/hour and 9.8 mg/dl respectively. Chest X-Ray reveals small bilateral pleural effusions and an enlarged cardiac silhouette. Transthoracic echocardiography is notable for pericardial enhancement anteriorly adjacent to the right ventricle and a small pericardial effusion. Estimated ejection fraction (EF) noted to be at 60%. Cardiac MRI performed is shown below (Fig A and B).
Figures A & B
Which of the following is the most likely diagnosis in this patient?
Show Answer
The correct answer is: A. NOD2- associated autoinflammatory disease (NAID)
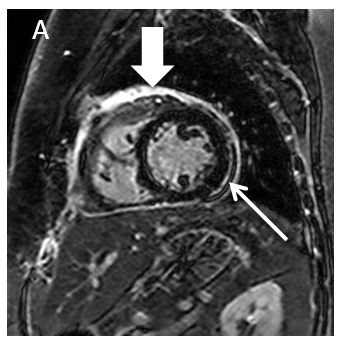
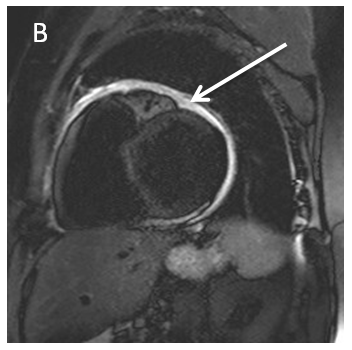
A. NAID represents a sporadic autoinflammatory disorder that is primarily characterized by episodic self-limiting fever, dermatitis, inflammatory polyarthritis and recurrent pericarditis1. The dermatitis is described as erythematous plaques, patches and macules, as seen in the case presented above2. Patients with NAID can also experience gastrointestinal symptoms, sicca-like symptoms and recurrent chest pain. Acute phase reactants are often times elevated, autoantibodies are absent, and NOD2 gene mutations are associated with the disease1. MRI often will show features of pericarditis, such as pericardial effusion and pericardial enhancement as depicted in Figures A & B.
Fig A. Fat suppressed delayed enhancement MRI imaging showing marked pericardial enhancement (thick arrow) and a small pericardial effusion (thin arrow) suggesting pericarditis.
Fig B. T2 STIR imaging showing marked pericardial enhancement (arrow) suggesting pericarditis on cardiac MRI.
B. Familial Mediterranean fever (FMF) is a disorder characterized by sporadic, unpredictable attacks of fever and serosal inflammation3. The initial attack usually occurs in childhood. The typical manifestations of the disease are recurrent attacks of severe pain and fever that last approximately three days. In between attacks, patients feel entirely well. The rash associated with this disorder is an erysipelas-like skin lesion. The lesion is tender, raised and erythematous, and occurs on the lower leg, ankle or foot, very different from the rash seen in NAID3. The estimated incidence of pericarditis in patients with FMF is roughly 0.7 percent3. FMF most commonly affects patients from the Mediterranean region with an observed disease rate of roughly 1 in 500. Diagnosis is primarily made on clinical grounds and response to colchicine4.
C. Postpericardiotomy syndrome occurs in patients post cardiac surgery. It is characterized by pericarditis with chest pain, pericardial effusion, fever, leukocytosis and a pericardial friction rub5,6. The diagnosis of postpericardiotomy syndrome depends upon the characteristic clinical picture, which usually appears about one to several weeks after surgery or cardiac injury. In a cohort of 360 consecutive patients undergoing cardiac surgery, 54 patients (15%) developed postpericardiotomy syndrome. The most common findings on diagnostic testing were pericardial effusions (89%) and elevated C-reactive protein or erythrocyte sedimentation rate (74%)7.
D. Camptodactyly arthropathy coxa vara pericarditis (CACP) syndrome is a rare condition principally characterized by congenital or early-onset camptodactyly (flexion contraction at the PCP joint) and childhood-onset non-inflammatory arthropathy, coxa vara deformity or other dysplasia associated with progressive hip disease and pericarditis8,9. The above patient does not exhibit any of these features; furthermore her disease onset was in adulthood.
E. Systemic Lupus Erythematous (SLE) can be associated with pericardial involvement. Pericardial effusion is the most common type of echocardiographic abnormality found in SLE with a reported prevalence rate anywhere from 21-49 percent10,11. Pericarditis is either acute or recurrent, often occurs when SLE is active, and is seen in approximately 25%of patients12. The above case is distinct from SLE in that the patient does not exhibit the common features seen in SLE such as malar or discoid rash, photosensitivity, mouth sores, renal, and hematological involvement.
References
Yao Q, Zhou L, et al. A new category of autoinflammatory disease associated with NOD2 gene mutations. Arthritis Res Ther. 2011; 13(5): R148.
Yao Q, Su LC, et al. Dermatitis as a characteristic phenotype of a new autoinflammatory disease associated with NOD2 mutations. J Am Acad Dermatol. 2013;68(4):624-631.
Kees S, Langevitz P, et al. Attacks of pericarditis as a manifestation of familial Mediterranean fever (FMF). QJM. 1997;90(10):643
Petrushkin H, Stanford M, et al. Clinical Review: Familial Mediterranean Fever-An Overview of Pathogenesis, Symptoms, Ocular Manifestations, and Treatment. Ocul Immunol Inflamm. 2015 Aug 24:1-9.
Imazio M, Brucato A, et al. Postpericardiotomy syndrome: a proposal for diagnostic criteria. J Cardiovasc Med (Hagerstown). 2013 May;14(5):351-3.
Imazio M and Hoit BD. Post-cardiac injury syndromes. An emerging cause of pericardial diseases. Int J Cardiol. 2013 Sep 30;168(2):648-52.
Imazio M, Brucato A, et al. Contemporary features, risk factors, and prognosis of the post-pericardiotomy syndrome. Am J Cardiol. 2011 Oct;108(8):1183-7.
Bahabri SA, Suwairi WM, et al. The camptodactyly-arthropathy-coxa vara-pericarditis syndrome: clinical features and genetic mapping to human chromosome 1. Arthritis Rheum. 1998;41 (4): 730-5.
Kakkar RM, Soneji S, et al. Camptodactyly-arthropathy-coxa vara-pericarditis syndrome: important differential for juvenile idiopathic arthritis. J Clin Imaging Sci. 2013 Jun 29;3:24.
Doria A, Iaccarino L, et al. Cardiac involvement in systemic lupus erythematosus. Lupus. 2005; 14:683.
Moder KG, Miller TD, Tazelaar HD. Cardiac involvement in systemic lupus erythematosus. Mayo Clin Proc. 1999;74(3):275.
Tincani A, Rebaioli CB, Taglietti M, Shoenfeld Y. Heart involvement in systemic lupus erythematosus, anti-phospholipid syndrome and neonatal lupus. Rheumatology (Oxford). 2006; 45 Suppl 4:iv8.