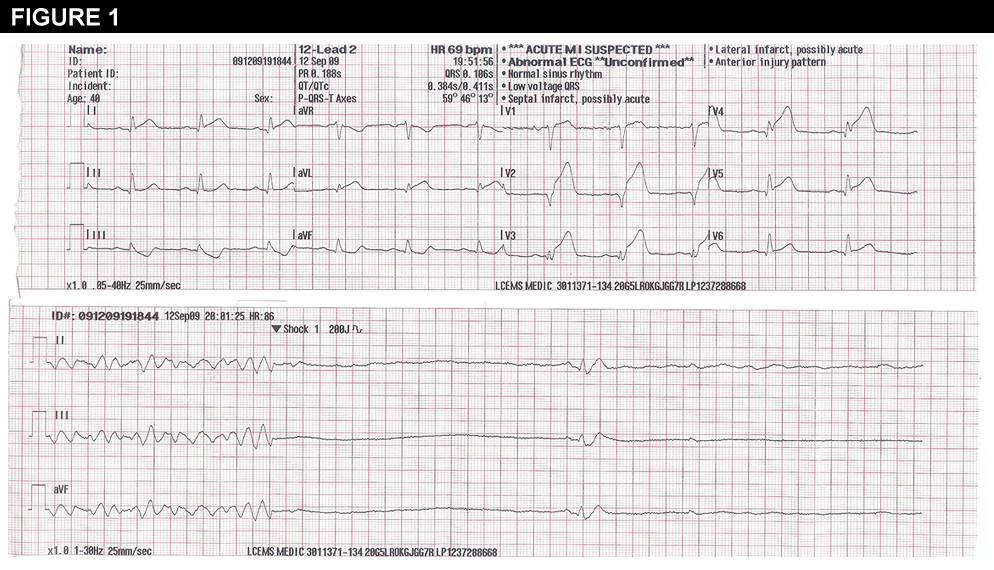
A 66 year old man with no prior medical history presented to the hospital with chest discomfort that began 3 hours prior to hospital presentation. In the field, EMS transmitted an ECG to the emergency department (Figure 1) that demonstrated ST-elevation in the anterior distribution. He had ventricular tachycardia en route that required defibrillation and a short course of cardiopulmonary resuscitation. Aspirin, intravenous heparin, clopidogrel and IV amiodarone was administered en route.
Figure 1
The patient was taken directly to the cardiac catheterization laboratory and was noted to have 100% proximal left anterior descending (LAD) occlusion. He underwent emergent percutaneous intervention to the LAD and was noted to have an ejection fraction of 15% by ventriculography. He was taken to the coronary care unit (CCU) for post-procedural care. Two hours post procedure, while clinically stable and asymptomatic, he had an episode of spontaneous ventricular fibrillation, which required external defibrillation.
Based on the above information, the next step in care would be:
Show Answer
The correct answer is: B. Continue beta blockers, aspirin, high-dose statin, and clopidogrel.
The patient presented with an acute coronary syndrome with high-risk anatomy (anterior infarction) and malignant ventricular arrhythmias. The arrhythmias occurred in the setting of an acute myocardial infarction and thus was secondary to this process. While the concept of acute stent thrombosis is reasonable, the absence of angina symptoms or a description of ongoing ST-elevation on ECG makes this an unlikely scenario.
While ICD therapy has shown a mortality benefit in the setting of malignant ventricular arrhythmias (primary and secondary prevention), this is clearly a reversible cause and would be a Class III indication by ACC/AHA/HRS guidelines.(1-4) Malignant ventricular arrhythmias that arise in the peri-infarction setting have not been shown to affect arrhythmic mortality post-infarction but do suggest poor prognosis (commonly due to pump failure) often unrelated to arrhythmic risk.(5-7) Outside of the peri-infarction period, non-sustained ventricular arrhythmias are considered a high risk feature and warrant further risk stratification (electrophysiology study) in the setting of moderate LV dysfunction (EF 35-40%).(3,8) The absence of mortality benefit from ICD therapy through day 40 post-myocardial infarction has been established and represents a Class III indication.(9) The utilization of a wearable defibrillator may be reasonable in the setting of high risk arrhythmia features post-myocardial infarction but no definitive data exist. In this case, the early presentation of ventricular arrhythmias within the reperfusion "window" does not imply an increased arrhythmia risk or need for an immediate ICD.
References
Epstein, AE, DiMarco, JP, Ellenbogen, KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: Executive Summary Circulation 2008; 117:2820-2840.
Moss AJ, Hall WJ, Cannom DS, et al, for the Multicenter Automatic Defibrillator Implantation Trial Investigators. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med 1996; 335:1933-40.
Buxton AE, Lee KL, Fisher JD, et al, for the Multicenter Unsustained Tachycardia Trial Investigators. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med 1999; 341:1882-90.
Moss AJ, Zareba W, Hall WJ, et al, for the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002; 346:877-83.
Nicod P, Gilpin E, Dittrich H, et al. Late clinical outcome in patients with early ventricular fibrillation after myocardial infarction. J Am Coll Cardiol 1988; 11:464-70.
Newby KH, Thompson T, Stebbins A, Topol EJ, Califf RM, Natale A, for the GUSTO Investigators. Sustained ventricular arrhythmias in patients receiving thrombolytic therapy: incidence and outcomes. Circulation 1998; 98:2567-73.
Al-Khatib SM, Stebbins AL, Califf RM, et al. Sustained ventricular arrhythmias and mortality among patients with acute myocardial infarction: results from the GUSTO-III trial. Am Heart J 2003; 145: 515-21.
Cheema, AN, Sheu,K, Parker, M, et al. Nonsustained Ventricular Tachycardia in the Setting of Acute Myocardial Infarction Tachycardia Characteristics and Their Prognostic Implications. Circulation 1998; 98:2030-2036.
Hohnloser SH, Kuck KH, Dorian P, et al. Prophylactic Use of an Implantable Cardioverter-Defibrillator after Acute Myocardial Infarction. N Engl J Med 2004; 351:2481-8.