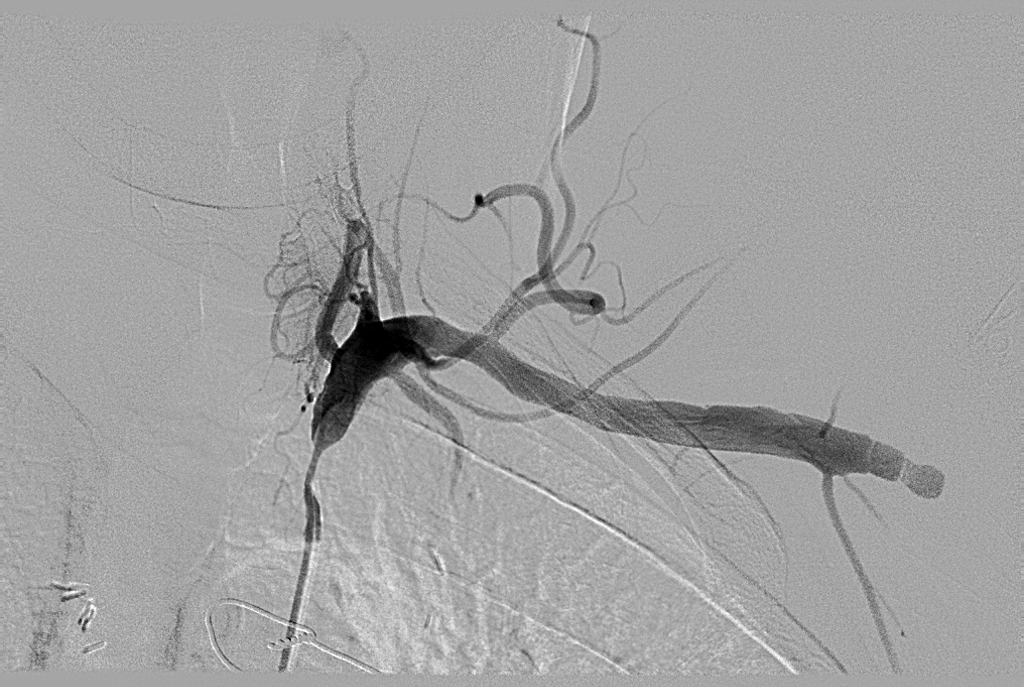
A 44-year-old gentleman is referred to you for chest pain, left arm claudication and exertional dyspnea four years after two-vessel coronary artery bypass graft (CABG) surgery using left internal mammary artery-to-left anterior descending artery (LIMA-to-LAD) and right internal mammary artery-to-ramus intermedius artery (RIMA-to-ramus); other significant medical history includes coronary artery disease (CAD), myocardial infarction, tobacco abuse, hypertension, and dyslipidemia. His stress test is strongly positive. Cardiac catheterization reveals stable multivessel native CAD, preserved left ventricular systolic function, and 80-90% proximal left subclavian artery concentric stenosis that functionally occludes his LIMA-to-LAD graft. Intra-arterial nitroglycerin injection prompted retrograde flow extending from the LAD via the LIMA graft into the left subclavian artery.
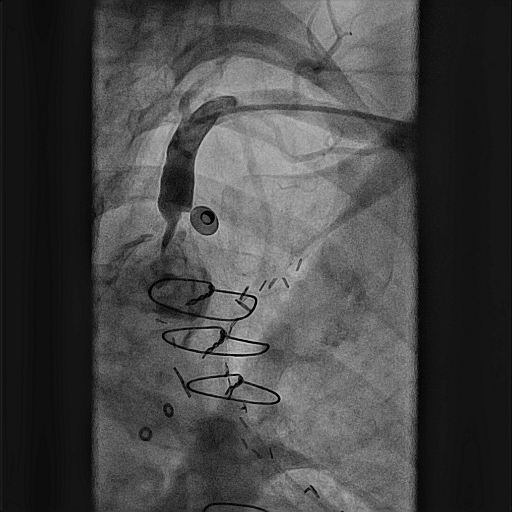
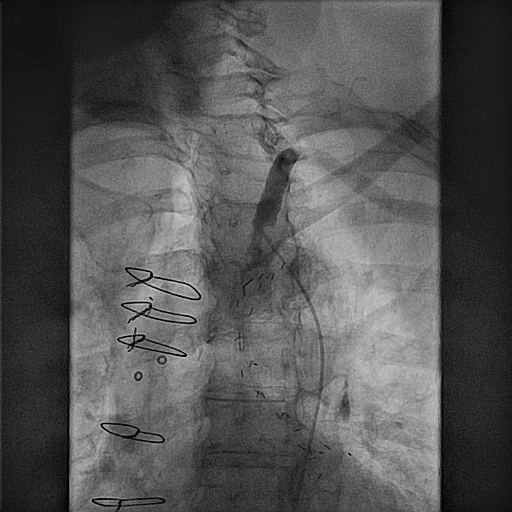
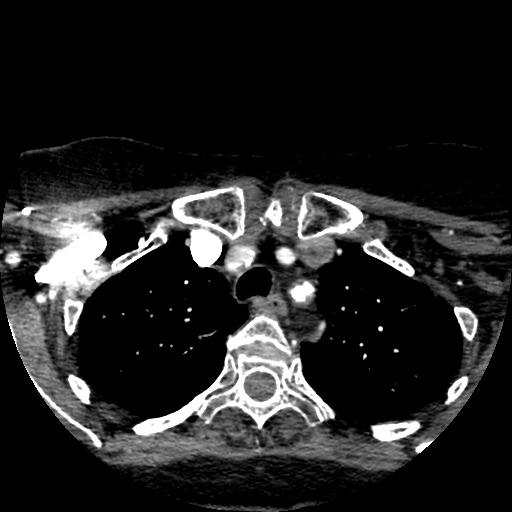
Later, a 79-year-old lady is referred to you for chest pain radiating into the jaw, both arms and the back, as well as dyspnea with exertion; other significant medical history includes CAD, remote five-vessel CABG with unknown anatomy status post percutaneous transluminal angioplasty, and drug-eluting stent implantation to the left main coronary artery and mid left circumflex artery, ischemic cardiomyopathy, diabetes mellitus, peripheral vascular disease, hypothyroidism, and dyslipidemia. Her stress test is also positive. Cardiac catheterization reveals multivessel native CAD, and 80-90% calcified ostial left subclavian artery stenosis with a significant pressure gradient across the lesion.
Review both patients' angiography films as well as the second patient's computed tomography (CT) imaging (Figures 1-4).
Figure 1
Figure 2
Figure 3
Figure 4
Which of the following statements describes the best approach to treat these patients' symptoms?
Show Answer
The correct answer is: E. Percutaneous transluminal angioplasty with subclavian artery stent implantation.
Coronary-subclavian steal syndrome (CSSS) is a rare cause of post-CABG myocardial ischemia. Harjola and Valle first described this clinical entity in 1974, and reports have increased as LIMA grafting has become standard of care in CABG procedures.1,2 Overall incidence, however, remains less than 1%.3
Proximal atherosclerosis of the left subclavian artery inverts the normal pressure gradient between the subclavian and the downstream LIMA-to-LAD graft, leading to ischemia as the subclavian "steals" blood supply from the coronary arteries via retrograde filling. Symptoms include angina pectoris, myocardial infarction, neurologic dysfunction, and even ventricular tachycardia.4
Atherosclerotic disease is the most common cause of CSSS, as in the two patients described above. Other etiologies include vasculitis, congenital abnormalities, thoracic outlet syndrome, and scarring secondary to previous vascular surgery. CSSS should always be considered when patients present with recurrent angina after CABG, especially if there are different blood pressures between the left and right arms on physical examination.5 Radial and ulnar pulses may also be weak or absent.
Noninvasive imaging modalities to diagnose CSSS include duplex arteriography, CT and magnetic resonance; however, direct subclavian angiography remains the gold standard for diagnosis.
Treatment of CSSS is evolving. Surgical correction with aorto-subclavian, carotid-subclavian or axilo-axilar bypass was the traditional approach.6 More recently, percutaneous transluminal angioplasty with subclavian artery stent implantation has been described with excellent results.7,8 Stent implantation is considered superior to balloon angioplasty due to high rates of restenosis with the latter. Benefits of angioplasty include minimal invasiveness, fewer complications, shorter length of hospital stay and avoidance of general endotracheal anesthesia; detriments include increased restenosis versus surgery.
In the two cases described in this Patient Case Quiz, the lower-risk profile of angioplasty in the setting of the patients' multiple comorbidities and individual risk factors made this intervention the preferred choice. Figures 5-7 document both patients' post-intervention results. Both patients did well with resolution of symptoms after angioplasty and stent implantation.
Figure 5
Figure 6
Figure 7
References
Harjola PT, Valle M. The importance of aortic arch or subclavian angiography before coronary reconstruction. Chest 1974;66:436-8.
Horowitz MD, Oh CJ, Jacobs JP, et al. Coronary-subclavian steal: a cause of recurrent myocardial ischemia. Ann Vasc Surg 1993;7:452-6.
Takach TJ, Reul GJ, Gregoric I, et al. Concomitant subclavian and coronary artery disease. Ann Thorac Surg 2001;71:187-9.
Kursaklioglu H, Kose S, Iyisoy A, et al. Coronary-subclavian steal syndrome presenting with ventricular tachycardia. Yonsei Med J 2009;50:852-5.
Marshall Jr WG, Miller EC, Kouchoukos NT. The coronary-subclavian steal syndrome: report of case and recommendation for prevention and management. Ann Thorac Surg 1988;46:193-6.
Perier BA, Williams GM. Carotid-subclavian bypass: a decade of experience. J Vasc Surg 1990;12:716-23.
Song L, Zhang H, Li J, et al. Endovascular stenting vs. extrathoracic surgical bypass for symptomatic subclavian steal syndrome. J Endovasc Ther 2012;19:44-51.
Marques K, Ernst S, Mast G, et al. Percutaneous transluminal angioplasty of the left subclavian artery to prevent or treat the coronary-subclavian steal syndrome. Am J Cardiol 1996;78:687-90.