Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
A 16-year-old, competitive, African American male basketball player presents after "failing" the pre-participation 12-point American Heart Association (AHA) screening examination.1 During the course of evaluation, he mentions that he occasionally feels chest pain during high-intensity running drills, occasional "extra beats" at rest, and episodes of suddenly "passing out," without premonitory symptoms, at the free throw line when he raises his arms to shoot. His family history is negative for sudden cardiac death, aneurysms, deafness, seizure, sudden infant death syndrome, pacemaker, implantable cardioverter-defibrillator, or need for cardiac transplant. Physical examination reveals a tall, athletic-appearing male with the following characteristics: resting heart rate in the 50s, blood pressure (BP) of 120/70 mm Hg, normoactive precordium, and non-displaced point of maximal impulse (PMI). He has a normal S1, physiologic S2, and no murmurs, with good and equal peripheral pulses. Of note, there is no high-arched palate and no arachnodactyly.
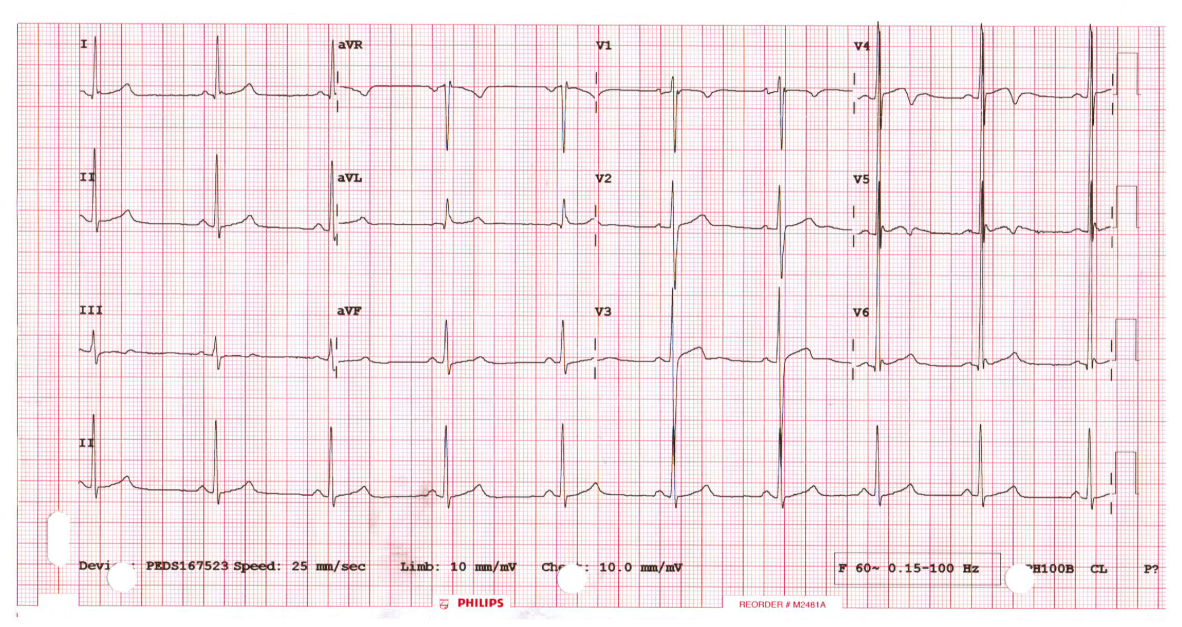
His electrocardiogram (ECG) is shown in Figure 1.
Figure 1
Selected transthoracic echocardiogram clips are shown in Videos 1 and 2.
Video 1
Video 2
A Holter monitor, obtained due to resting bradycardia and complaints of extra beats and syncope, shows a predominance of sinus rhythm, with rate varying from a low of 37 BPM during sleep (without sinus pauses nor atrioventricular block) to a maximum of 180 BPM during a pick-up game of basketball. At rest, there is a 5 beat run of wide complex tachycardia at 150 BPM.
Due to the competitive nature of this athlete and his symptoms, an exercise stress test is obtained. He runs through Stage 4 of the Bruce protocol, during which he is asymptomatic, achieving 14 METS, with normal heart rate and BP response, and without ST changes or ectopy.
Which of the following statements describes the next best steps in further testing or intervention for this patient?
Show Answer
The correct answer is: A. Order coronary computed tomography angiography (CCTA) and, if concerning, discuss surgical intervention.
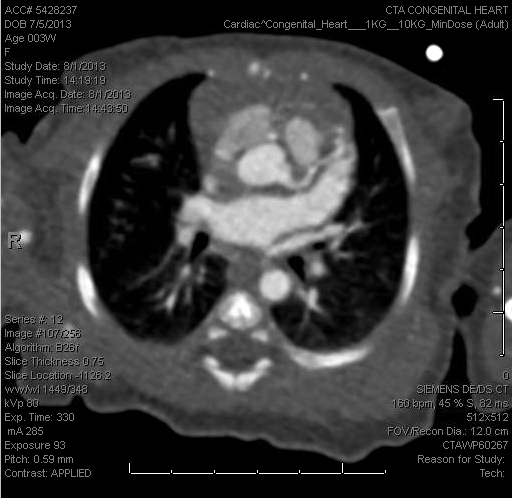
The transthoracic echocardiogram hints at the diagnosis, which is confirmed by CCTA and upon surgical inspection. Based on careful review of the transthoracic echocardiogram, the left circumflex is seen originating from the right sinus of Valsalva, despite initially appearing to originate from its usual orifice (Video 1). However, careful review shows the anomalous origin of the left circumflex from the right sinus of Valsalva, which is then visualized crossing posterior to the aortic root (Video 2), and is traced through its course in the atrioventricular groove, at the level of the mitral annulus. This finding was confirmed by CCTA (Figure 2) and was validated by intraopertive transesophageal echocardiography (TEE) (Video 3) and visual inspection at surgery.
Figure 2
Video 3
This type of anomalous aortic origin of the left coronary artery (AAOLCA), where the left circumflex originates from the right sinus or right coronary artery, is the second most common type reported in adults (0.37%),2 after dual origin of the left coronary artery (0.41%). A more recent study of AAOCA in children (median age at diagnosis = 10.2 years; 64% male, N = 196 living patients), describes anomalous aortic origin of the right coronary artery (AAORCA) in 144 patients (73%) and AAOLCA in 51 patients (26%).3 In this study, more than half of these patients presented with chest pain, most of whom had AAORCA. Two patients presented with sudden cardiac death (SCD), one with AAOLCA and one with a single ostium.
In general, anomalous left circumflex artery from the right coronary cusp has been considered a benign variant, with less association with chest pain, syncope, arrhythmia, and atherosclerosis4-6 in spite of its acute angulation and retro-aortic course. Nonetheless, cardiac symptomatology due to myocardial ischemia in the territory of the LCA in the absence of atherosclerosis has been reported with this anomaly, prompting surgical re-implantation of the coronary with subsequent improvement in fractional flow reserve.6 Angina, syncope, and SCD have all been reported with this defect, prompting intervention in those with cardiac symptoms.7 There have been reports of myxomatous mitral valves in association with AAOCA.8
Most concerning of all these symptoms of AAOCA, is that of SCD or sudden cardiac arrest (SCA).9 However, while SCD and symptoms are well publicized, the true incidence and prevalence of AAOCA is unknown, as many may be "silent." In fact, Basso and colleagues remark on the normalcy of the appearance of the ECG, the lack of findings by exercise stress test, and the very unfortunate possibility of false negative findings on screening echocardiograms, in which the origins of the coronary arteries may not always be defined.9
Is surgical correction/palliation of AAOCA appropriate? Certainly, for those with an intramural or inter-arterial course, with resultant possible compression during exercise, surgery appears to be indicated. In the case of the left circumflex arising from the right, the answer is not always clear. The acute angulation causes concern for compression and potentially results in a narrow or slit-like orifice, but this is difficult to predict. Jo and colleagues described intimal thickening, fragmentation, and random arrangement of elastic fibers along with degeneration of medial smooth muscle cells and an increase in medial stromal substance on a pathological specimen of the coronary artery they re-implanted.10 Medium-term results of a small cohort of AAOCA indicates that the majority of patients experience relief and are able to resume activity.11
This patient presents a common scenario: occasional ill-defined chest pain,12 palpitations at rest with bradycardia,13,14 and syncope, commonly occur in fit athletes.14,15 In fact, in a situation in which hundreds of athletes are being screened, these symptoms may possibly have been inadvertently ignored without strict adherence to the 12-point AHA screening tool, and he could have been allowed to play without further intervention.
Is it serendipitous that the coronary origins are found to be anomalous in this athlete? Perhaps, but his constellation of symptoms were concerning enough to prompt further investigation and confirmation by CCTA, a tool which is proving to have great promise in the area of evaluating AAOCA.16,17
Did this patient require surgery, and if so, will it improve his course? This is the fodder of future registries and studies,3 which health care providers should all strongly support in efforts to level the playing field and provide safe play for our young athletes.
References
Mahle WT, Sable CA, Matherne PG, Gaynor JW, Gewitz MH. Key concepts for the evaluation and screening of heart disease in children and adolescents: a scientific advisory from the American Heart Association. Circulation 2012;125:2796-801.
Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: Diagnosis, angiographic class, and clinical significance. Radiology 1979;130:39-47.
Poynter JA, Williams WG, McIntyre S, Brothers JA, Jacobs ML; Congenital Heart Surgeons Society AAOCA Working Group. Anomalous aortic origin of a coronary artery: a report from the Congenital Heart Surgeons Society Registry. World J Pediatr Congenit Heart Surg 2014;5:22-30.
Mohsen GA, Mohsin KG, Forsberg M, Miller E, Taniuchi M, Klein AJP. Anomalous left circumflex artery from the right coronary cusp: a benign variant? J Invasive Cardiol 2013;25:284-7.
Samarendra P, Kumari S, Hafeez M, Vasavada BC, Sacchi TJ. Anomalous circumflex coronary artery: benign or predisposed to selective atherosclerosis. Angiology 2001;52:521-6.
Coceani M, Ciardetti M, Pasanisi E, et al. Surgical correction of left coronary artery origin from the right coronary artery. Ann Thorac Surg 2013;95:e1-2.
Lim JC, Beale A, Ramcharitar S. Anomalous origination of a coronary artery from the opposite sinus. Nat Rev Cardiol 2011;8:708-16.
Imori Y, Murakami M, Tanaka M, Saito S. Anomalous origin of the right coronary artery with concomitant myxomatous mitral valve disease: a rare coexistence. BMJ Case Rep 2014;23:206351.
Basso C, Maron B, Corrado D, Thiene G. Clinical profile of congenital coronary artery with origin from the wrong sinus leading to sudden cardiac death in young competitive athletes. J Am Coll Cardiol 2000;35:1493-501.
Jo Y, Uranaka Y, Iwaki H, Matsumoto J, Koura T, Negishi K. Sudden cardiac arrest associated with anomalous origin of the right coronary artery from the left main coronary artery. Tex Heart J 2011;3:539-43.
Wittlieb-Weber CA, Paridon SM, Gaynor JW, Spray TL, Weber DR, Brothers JA. Medium-term outcome after anomalous aortic origin of a coronary artery repair in a pediatric cohort. J Thorac Cardiovasc Surg 2014;147:1580-6.
Friedman KG, Alexander ME. Chest pain and syncope in children: a practical approach to the diagnosis of cardiac disease. J Pediatr 2013;163:896-901.
Uberoi A, Stein R, Perez MV, et al. Interpretation of electrocardiograms in young athletes. Circulation 2011;124:746-57.
Lampert R. Evaluation and management of arrhythmias in the athletic patient. Prog Cardiovasc Dis 2012;54:423-33.
Hastings JL, Levine BD. Syncope in the athletic patient. Progr Cardiovasc Dis 2012;54:438-44.
Ashrafpoor G, Danchin N, Houyel L, Ramadan R, Belli E, Paul JF. Anatomical criteria of malignancy by computed tomography angiography in patients with anomalous coronary arteries with an interarterial course. Eur Radiol 2015;25:760-6.
Clark RA, Marler AT, Lin CK, et al. A review of anomalous origination of a coronary artery from an opposite sinus of Valsalva (ACAOS) impact on major adverse cardiovascular events based of coronary computerized tomography angiography: a 6-year single center review. Ther Adv Cardiovasc Dis 2014;8:237-41.