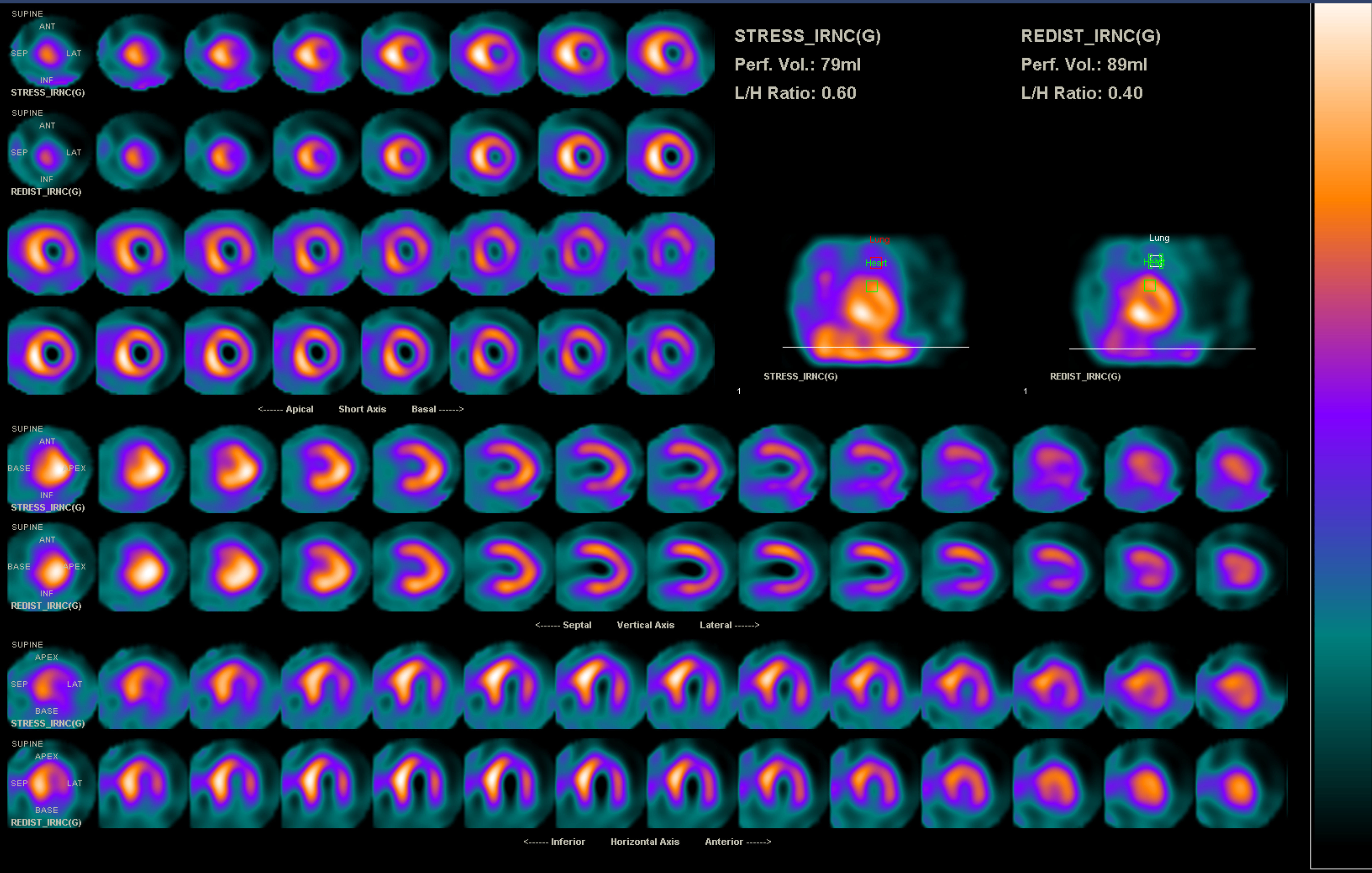
A 59-year-old woman, who gave birth to three children uneventfully and has only a history of mitral valve prolapse, presents to the emergency department with intermittent chest tightness and dyspnea on exertion with insidious onset and acute worsening over 2 weeks. A grade III/VI systolic murmur most prominent at the left sternal border and bilateral basal rales are noted on physical examination. Chest X-ray shows cardiomegaly with pulmonary edema; echocardiography reveals dilated left atrium and left ventricle with preserved ejection fraction, as well as moderate mitral and tricuspid regurgitation. A diagnosis of acute heart failure is made, and cardiac catheterization is performed to exclude coronary artery disease. Surprisingly, the opening of left coronary artery (LCA) could not be demonstrated by angiography. Instead, a huge right coronary artery (RCA) with collateralization to the left side is noted, with the vessel eventually draining into the right pulmonary artery (Video 1). Myocardial perfusion imaging reveals moderate reversible perfusion defect over anterior and anteroseptal wall (Figure 1).
Figure 1
Video 1
Which of the following statements is incorrect?
Show Answer
The correct answer is: A. This patient is diagnosed with an anomalous origin of the LCA from the pulmonary artery (ALCAPA), also known as Bland-White-Garland syndrome. Patients with this form of congenital heart disease (CHD) rarely survive into the adulthood and the syndrome has a male predominance.
Answer Options A and B: ALCAPA is a rare form of CHD that involves 1 in 300,000 live births, and most (90%) infants die within the first year of life. Among reported adult cases, females have a more than 2:1 predominance, and about two-thirds of patients had only minor complaints, such as palpitations, until they present with ventricular arrhythmia, syncope, or sudden cardiac death in their thirties.
Answer Option D: The generally proposed explanation of such curious time course is a 4-phase pathophysiology: the elevated neonatal pulmonary artery (PA) pressure and oxygenation levels provide sufficient antegrade perfusion of the LCA territory; as the ductus arteriosus closes and antegrade oxygenation decreases in early infancy, symptoms of myocardial ischemia develop. Survival into the adulthood depends on the development of collateral vessels from the RCA, and the flow is then reversed from the LCA into the PA. Finally, excessive shunting from the collaterals into the PA may produce a "coronary steal" from the RCA, which causes fatal arrhythmia or deterioration of heart function.
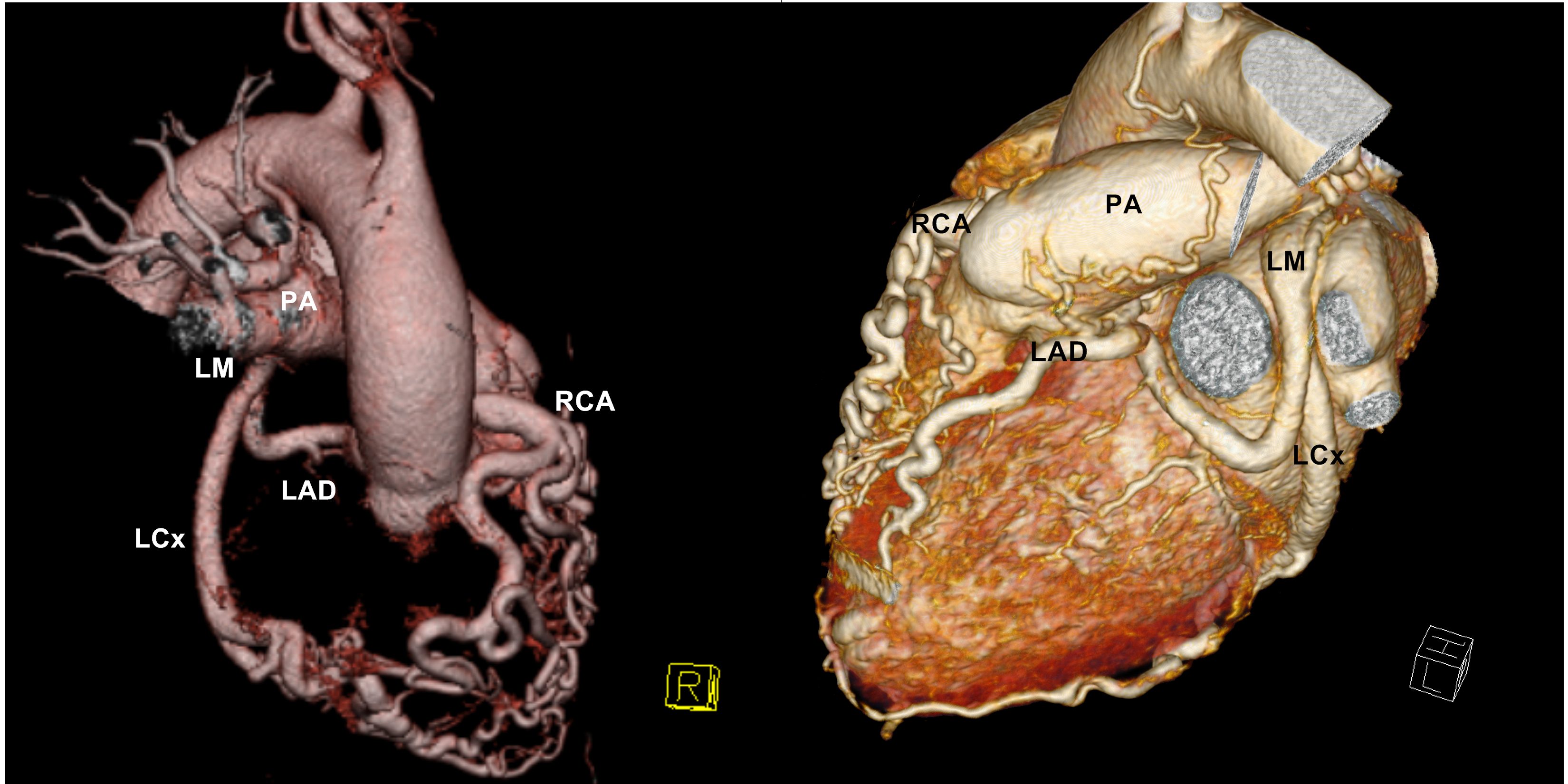
Answer Option C: Such pathophysiology also helps health care providers understand some objective signs of ALCAPA. Systolic murmur is common on physical examination; some patients even have a continuous or "to-and-fro" murmur localized to the left sternal border or apical region – probably related to the high-speed shunting of collaterals or ischemic mitral regurgitation. Echocardiography reveals signs such as retrograde LCA-to-PA flow, increased systolic pulsed wave Doppler flow at the RCA ostium, and prominent septal turbulent flow due to collateralization. Currently, the gold standard of diagnosis is still coronary angiography, but computed tomography and magnetic resonance imaging have emerged due to their noninvasiveness and high special resolution, as shown in our patient (Figure 2). If myocardial ischemia was demonstrated, either by MRI or myocardial perfusion imaging as in this patient, reconstruction of a dual coronary artery system is recommended. Direct implantation is usually difficult in the adult patients due to tissue rigidity. Instead, bypass grafting from the ascending aorta to the LCA and ligation of its origin at the PA are performed in this patient, and she is discharged free of symptoms.
Figure 2
References
Alsara O, Kalavakunta JK, Hajjar V, Alsarah A, Cho N, Dhar G. Surviving sudden cardiac death secondary to anomalous left coronary artery from the pulmonary artery: a case report and literature review. Heart Lung 2014;43:476-80.
Yau JM, Singh R, Halpern EJ, Fischman D. Anomalous origin of the left coronary artery Ffom the pulmonary artery in adults: a comprehensive review of 151 adult cases and a new diagnosis in a 53-year-old woman. Clin Cardiol 2011;34:204-10.
Ghaderi F, Gholoobi A, Moeinipour A. Unique echocardiographic markers of anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) in the adult. Echocardiography 2014;31:E13-5.
Ishikawa K, Funabashi N, Ozawa K, Takaoka H, Kobayashi Y. An anomalous left coronary artery branching off the pulmonary artery (Bland-White-Garland syndrome) diagnosed by 320 detector rows computed tomography. J Am Coll Cardiol 2015;65:A653.
Quah JX, Hofmeyr L, Haqqani H, et al. The management of the older adult patient with anomalous left coronary artery from the pulmonary artery syndrome: a presentation of two cases and review of the literature. Congenit Heart Dis 2014;9:E185-94.