A 27-year-old female with a past medical history significant for pericarditis presents to clinic to establish care for ongoing pericarditis management. She is 8 weeks pregnant, and continues to have symptoms. She was first diagnosed with pericarditis 3 months prior. She initially presented with persistent sharp substernal chest pain, made worse with inspiration. Physical exam with pericardial rub and Ewart's signs present. ECG with mild PR depressions (Figure 1), and echocardiogram with moderate circumferential pericardial effusion (Figure 2). She was initially started on ibuprofen 600mg three times daily, with moderate improvement in symptoms. Ibuprofen was subsequently increased to 600mg four times daily at a recent emergency department visit, given persistent symptoms. On presentation today, she continues to have sharp chest pain, worse with inspiration and lying flat. Vitals today show that she is afebrile, with heart rate of 89 beats per minute and blood pressure of 124/66 mmHg. Echocardiogram today shows largely resolved pericardial effusion. However, patient continues to have elevated inflammatory biomarkers. Ultrasensensitive C-Reactive Protein was 66.2 mg/L on initial presentation, and is 79.9 mg/L today. Westergren erythrocyte sedimentation rate was 42 mm/hr on initial presentation, and is 78 mm/hr today. She was recently seen by an obstetrician and told she is 8 weeks pregnant.
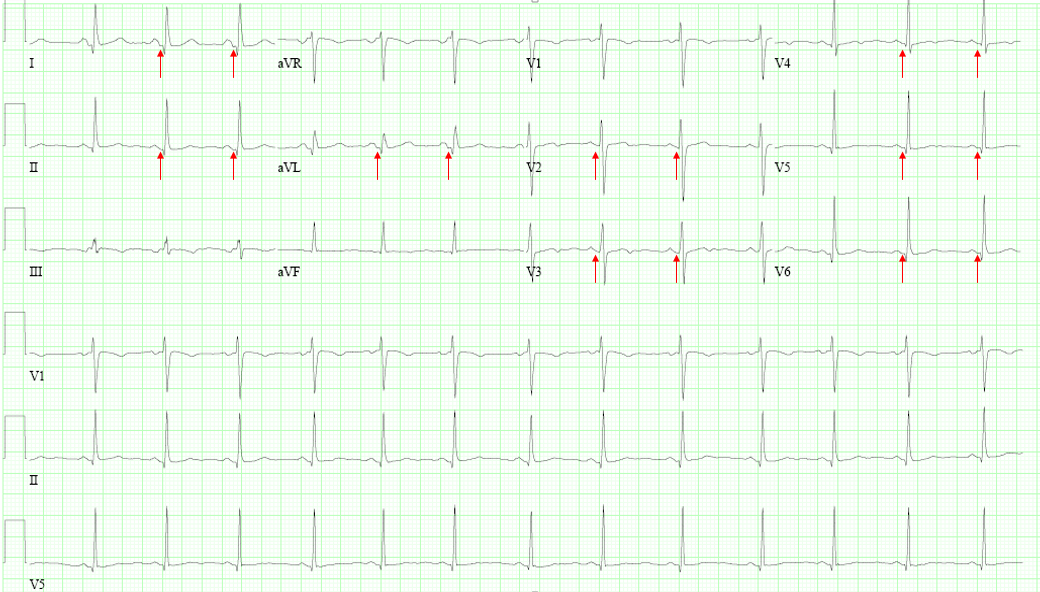
Figure 1: Arrows point to PR depressions
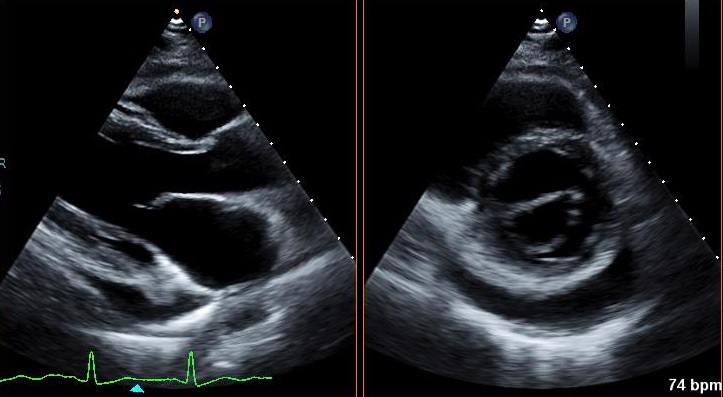
Figure 2: Transthoracic echocardiogram (left: parasternal long axis; right: parasternal short axis)
Which of the following is the best next step for managing this patient's pericarditis?
Show Answer
The correct answer is: C. Discontinue ibuprofen and start aspirin 650mg twice daily.
In this case presentation the patient continues to have evidence of active pericarditis (symptoms, elevated inflammatory biomarkers) despite ibuprofen therapy. It would be inappropriate to discontinue all anti-inflammatory therapy at this point in time (answer A). The optimal medication regimen to manage pericarditis during pregnancy is controversial. Unfortunately, very little evidence exists for this particular clinical scenario. The ACC and AHA do not have any guideline statements for situation either. However, the European Society of Cardiology (ESC) 2015 Guidelines for the diagnosis and management of pericardial disease do offer guiding principles.1 Generally, the ESC recommends high dose aspirin as first line therapy in the first 20 weeks of gestation, and then prednisone thereafter.
Compared to other anti-inflammatory medications, colchicine has very little data in pregnancy. It is currently not recommended for use in pregnancy (answer B and D). However, it should be noted that colchicine has been safely used in pregnancy in the treatment of Familial Mediterranean Fever.2,3 In these retrospective cohort studies, the rate of miscarriage is similar between women treated with colchicine and those treated without. However, given effective alternative therapies, colchicine should not be routine escalation of pericarditis management in pregnancy.
While little data exists specific to pericarditis and pregnancy, NSAIDs and aspirin have been studied in other inflammatory disease, and have a reasonably safe side effect profile during the first and second trimesters. Large cohort studies of national databases in Norway and Israel did not find any association between NSAID use in the first trimester and fetal birth defects.4,5 Aspirin is preferred over other NSAIDs because low dose aspirin (compared to other NSAIDs) is associated with reduced risk of preeclampsia, preterm birth, and intrauterine growth restriction in high risk pregnancies.6 However, it should be noted that most trials of aspirin in pregnancy use low-dose aspirin, as opposed to the high doses used for treatment of pericarditis. During the third trimester, NSAIDs should be avoided for risk of premature closure of the ductus arteriosus in the fetus. Answer D is incorrect because it uses ibuprofen as the NSAID.
Studies regarding prednisone use during pregnancy are mixed. While prednisone use is permissible throughout pregnancy (FDA pregnancy safety class B), some studies suggest that prednisone use during the first trimester is associated with increased risk of fetal cleft palate.7 Furthermore, complicating prednisone use during pregnancy are increased maternal risk of diabetes and hypertension.
Table 1: Proposed Medical Treatment of Pericarditis During Pregnancy
< 20 weeks pregnant
> 20 weeks pregnant
High dose aspirin
First choice
To be avoided
NSAID
Allowed
To be avoided
Prednisone
Allowed
Allowed
Colchicine
Controversial
Controversial
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Rabinovitch O, Zemer D, Kukia E, Sohar E, Mashiach S. Colchicine treatment in conception and pregnancy: two hundred thirty-one pregnancies in patients with familial Mediterranean fever. Am J Reprod Immunol 1992;28:245-6.
Ehrenfeld M, Brzezinski A, Levy M, Eliakim M. Fertility and obstetric history in patients with familial Mediterranean fever on long-term colchicine therapy. Br J Obstet Gynaecol 1986;94:1186-91.
Daniel S, Matok I, Borodischer R, et al. Major malformations following exposure to nonsteroidal antiinflammatory drugs during the first trimester of pregnancy. J Rheumatol 2012;39:2163-9.
van Gelder M, Roeleveld N, Nordeng H. Exposure to non-steroidal anti-inflammatory drugs during pregnancy and the risk of selected birth defects: a prospective cohort study. PLoS One 2011;6:e22174.
LeFevre M, United States Preventive Services Task Force. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2014;161:819-26.
Park-Wyllie L, Mazzotta P, Pastuszak A, et al. Birth defects after maternal exposure to corticosteroids: prospective cohort study and meta-analysis of epidemiological studies. Teratology 2000;62:385-92.